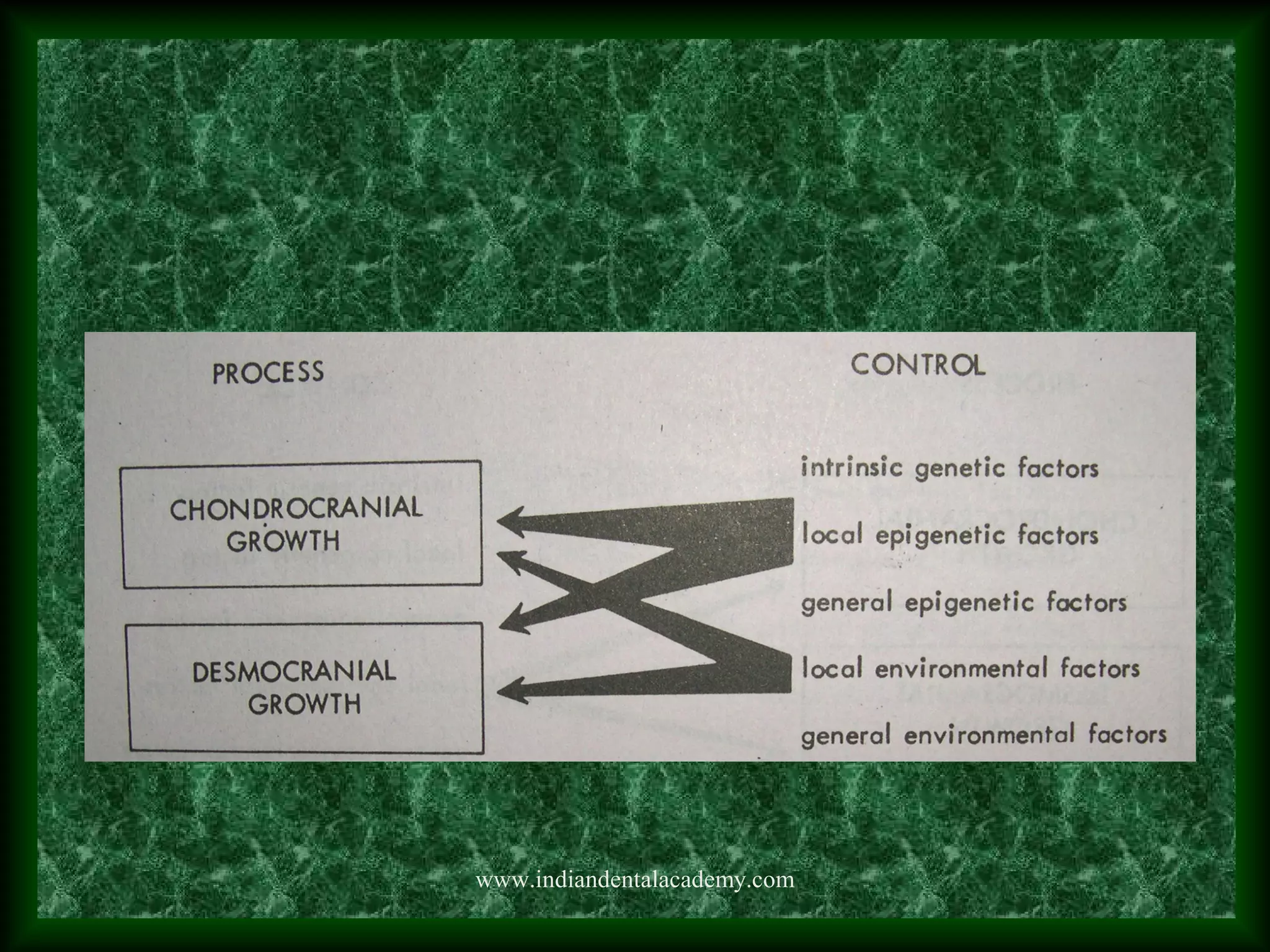
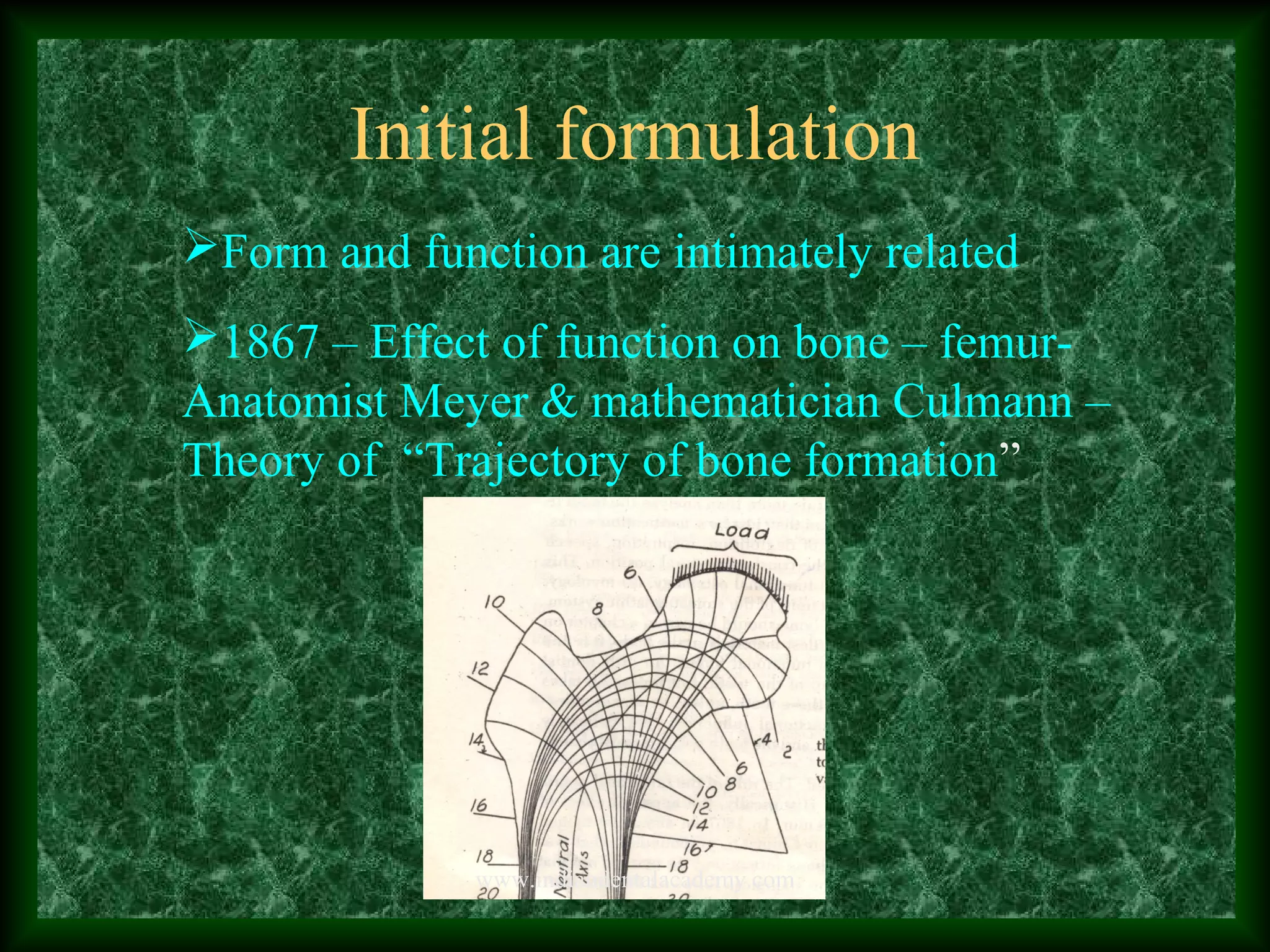
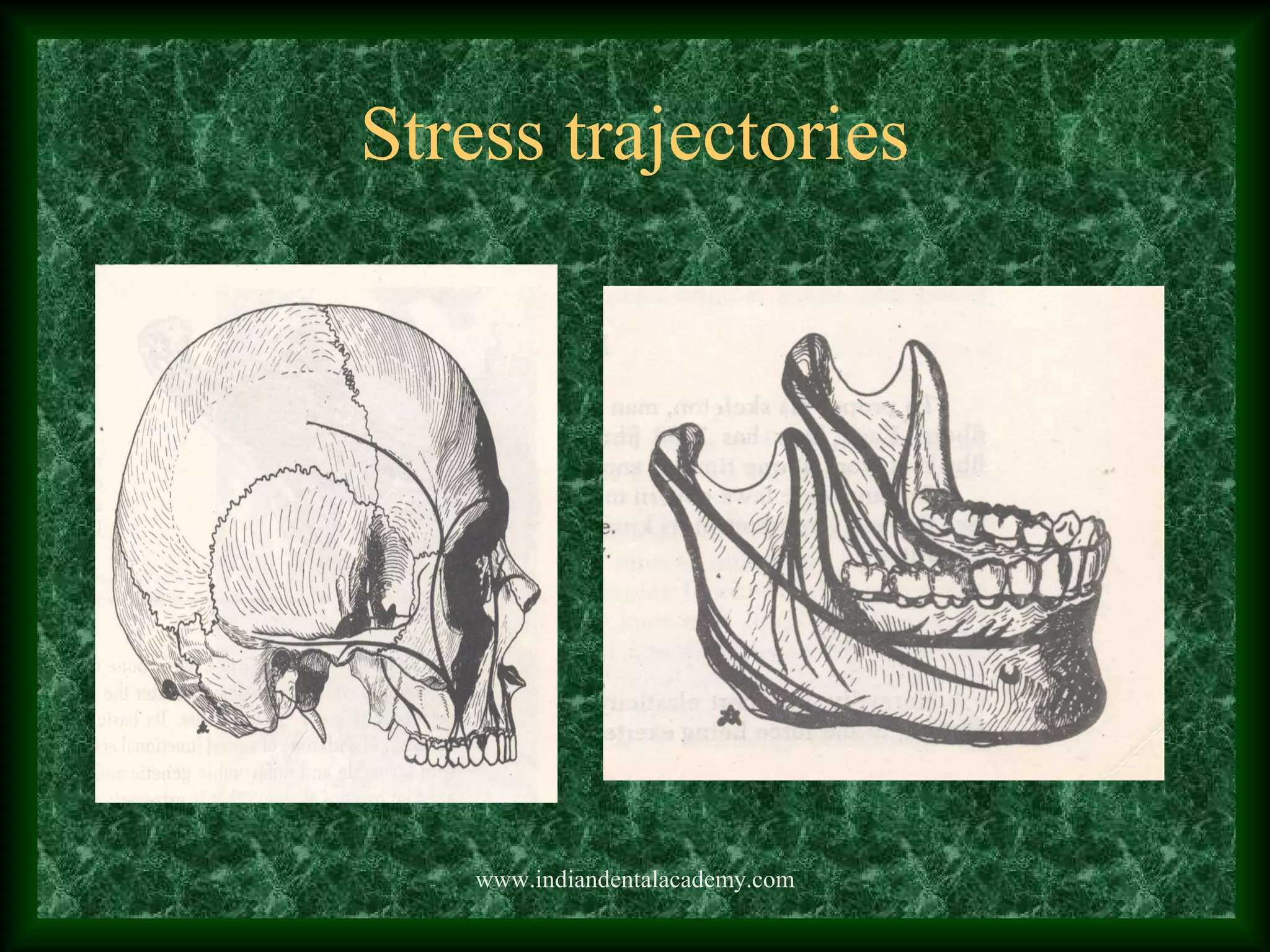

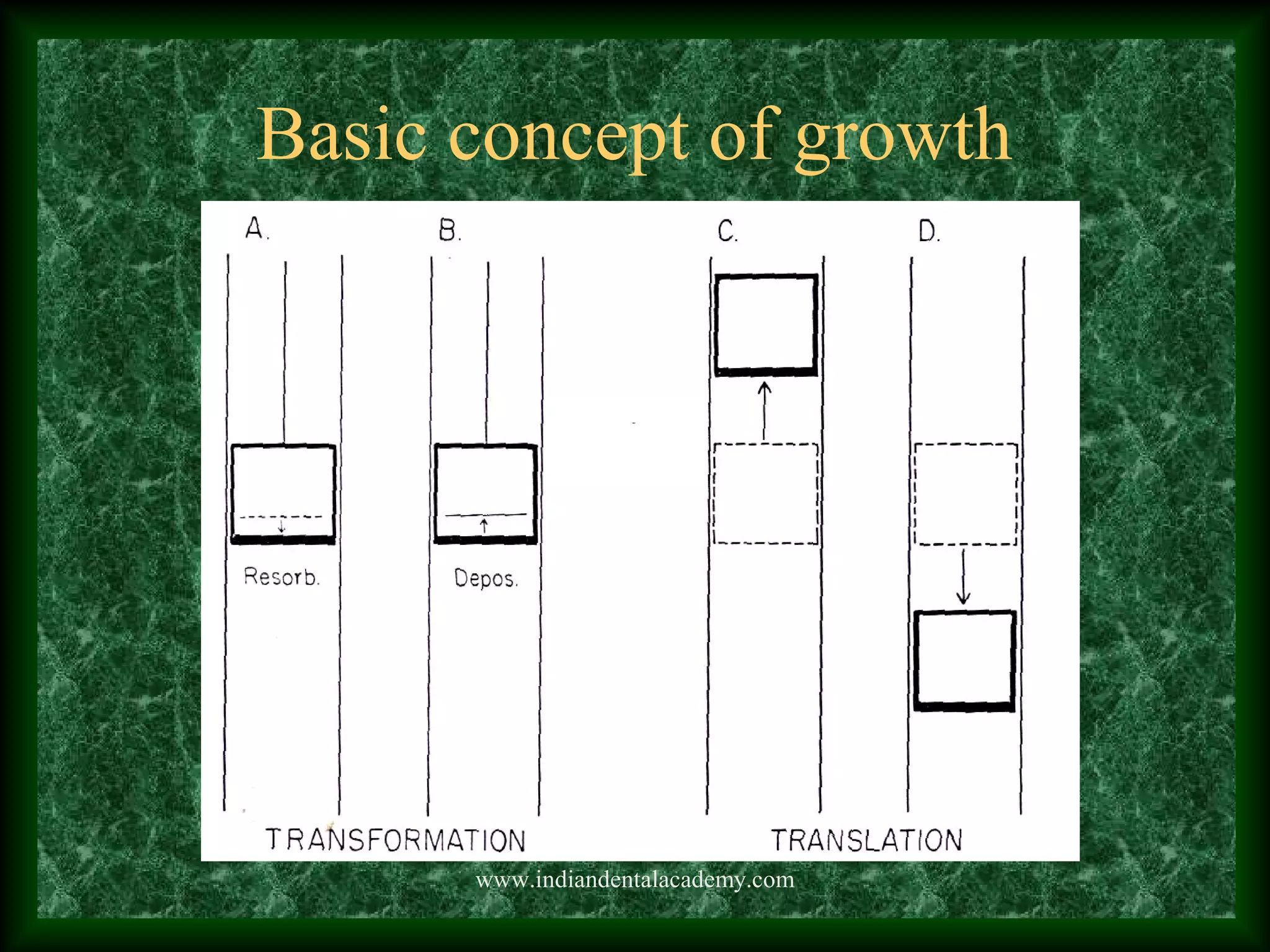
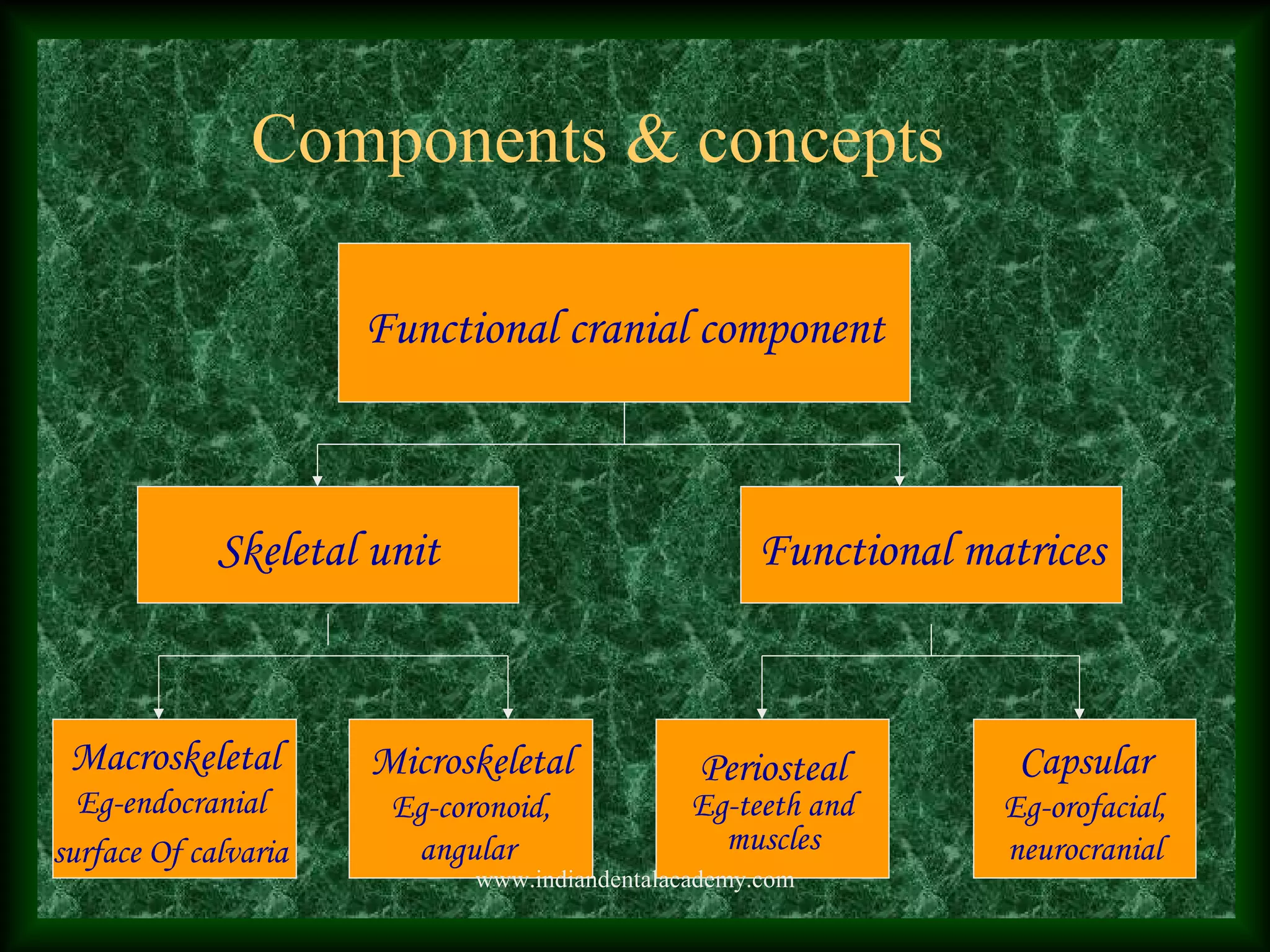


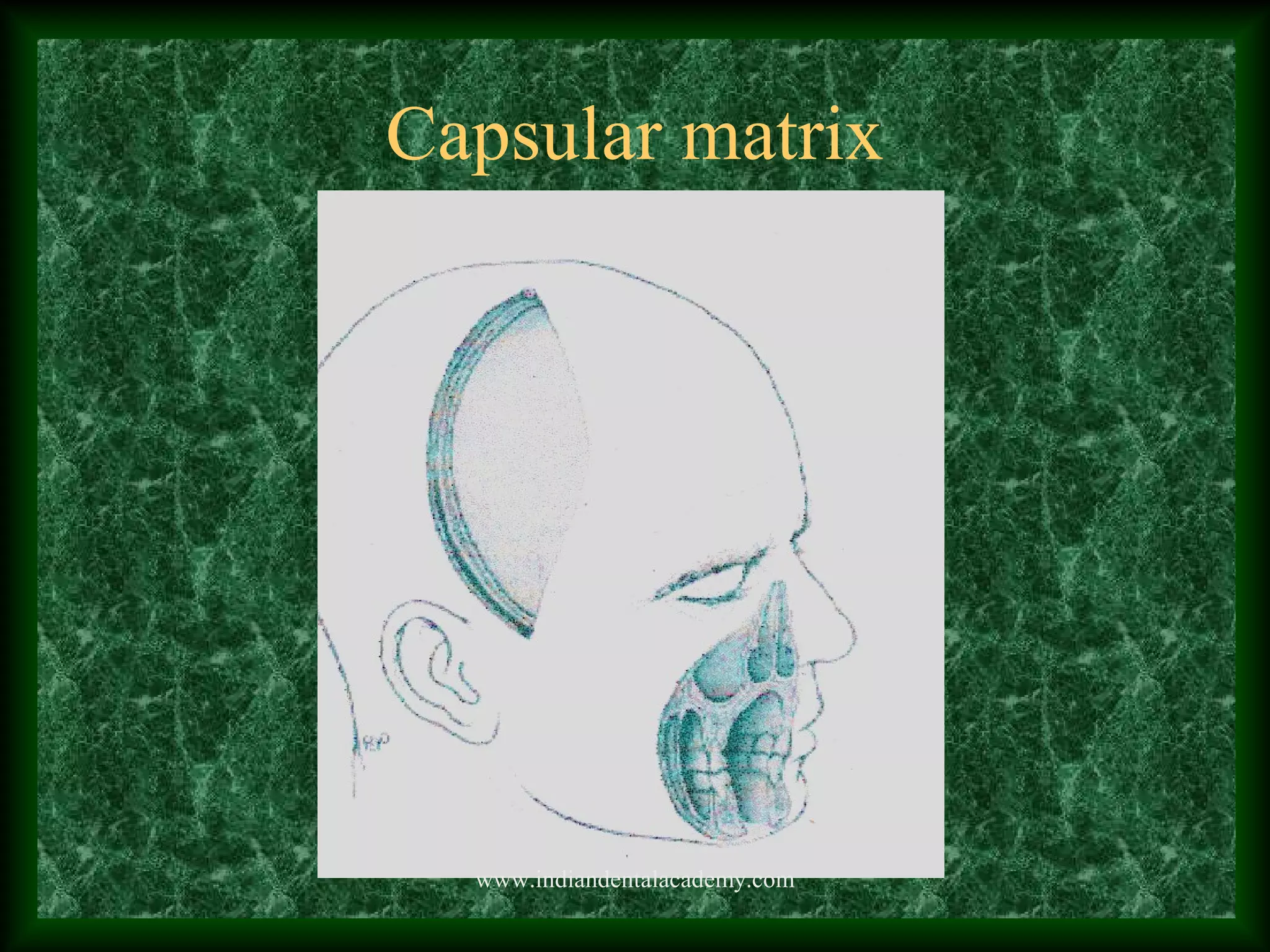
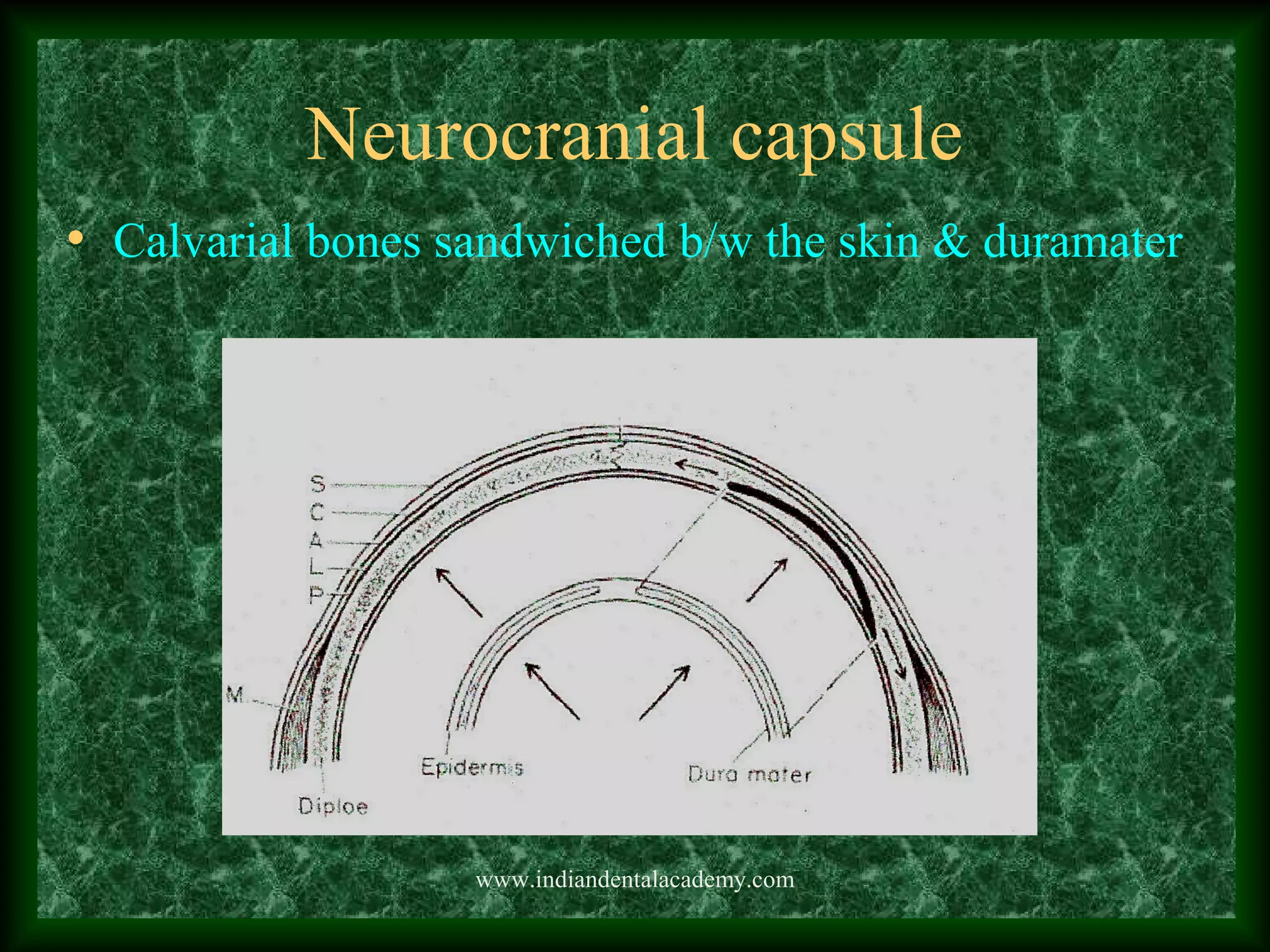


The functional matrix hypothesis proposes that the growth and development of skeletal tissues is a secondary response to functional demands imposed by non-skeletal tissues like muscles and organs. It was first formulated in the 1860s and developed by Melvin Moss in the 1960s. The hypothesis states that the craniofacial skeleton adapts and remodels according to mechanical forces from functional matrices like muscles, nerves and blood vessels. Growth occurs through transformation and translation of bones driven by the expansion of surrounding capsular matrices like the neurocranial and orofacial capsules. Clinical support includes mandibular growth changes after condylectomies and effects of airway dysfunction on facial development.






































































































