Download to read offline











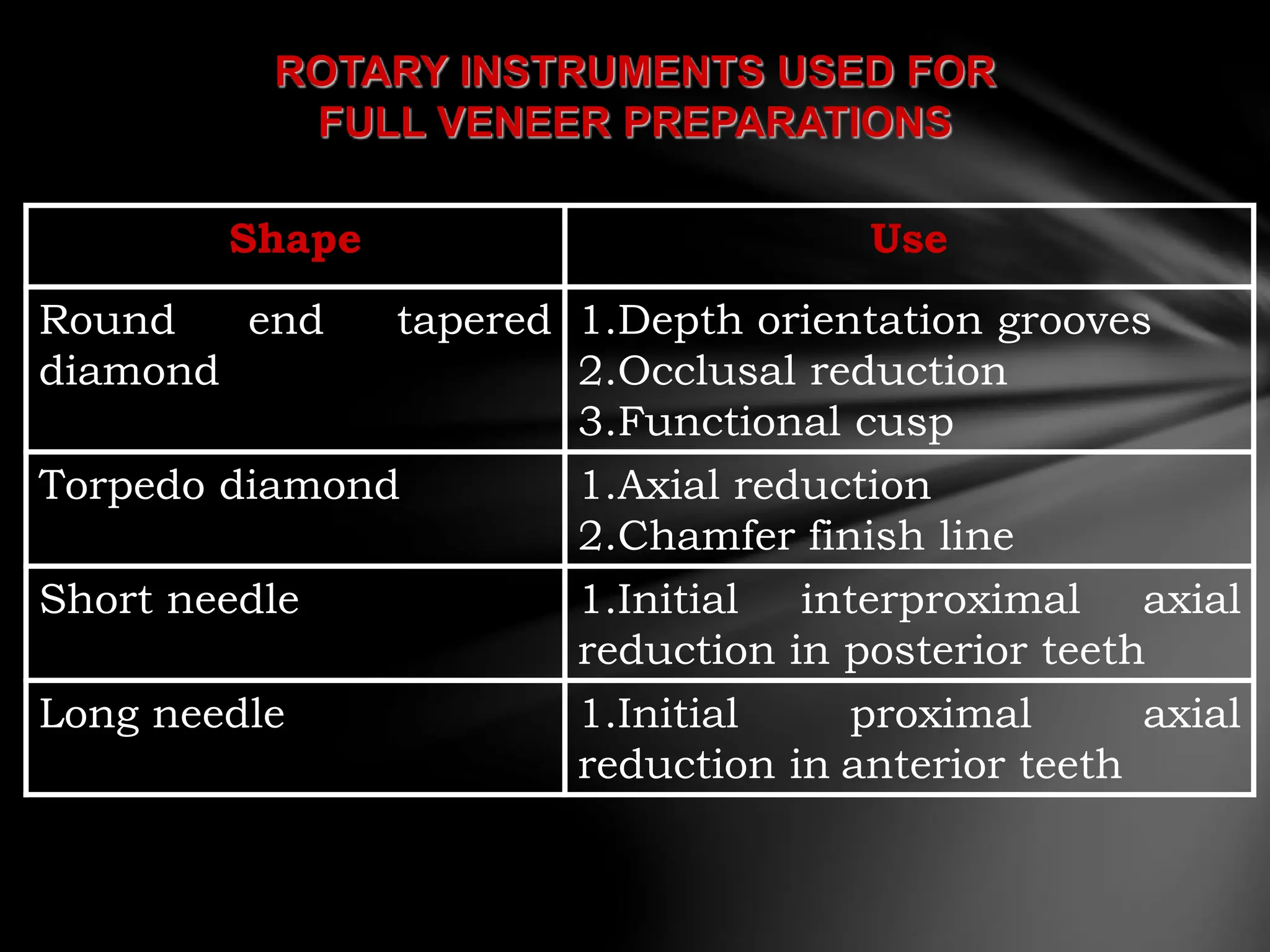





































































The document discusses the process of tooth preparation for full veneer crowns, defining key terms and concepts such as retention and resistance forms, various crown types, and the importance of specific measurements for tooth reduction. It outlines indications and contraindications for using full veneer crowns, along with advantages, disadvantages, and necessary armamentarium for the preparation process. Additionally, it reviews literature on retention factors related to different crown preparation techniques and provides references for further reading.



































































