Downloaded 527 times

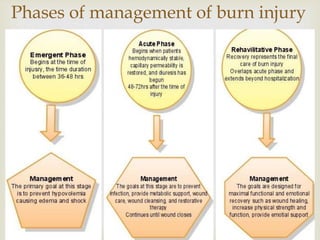
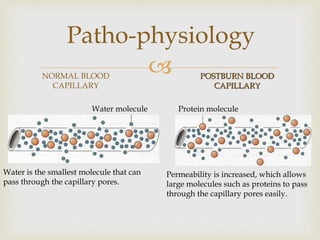
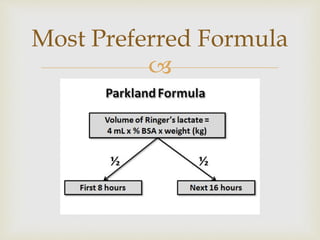

This document discusses fluid resuscitation for burn injuries. It notes that before 1940s, hypovolemic shock was a leading cause of death from burns but mortality has decreased with fluid resuscitation formulas. However, 50% of burn deaths in the first 10 days are still due to inadequate or inappropriate fluid management. The document then describes the pathophysiology of burn shock, standard resuscitation methods using formulas like Parkland formula, and complications that can arise like over-resuscitation. It emphasizes the importance of monitoring patients closely during resuscitation.
































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








