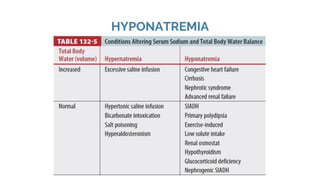
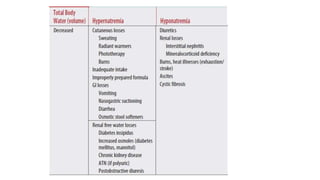
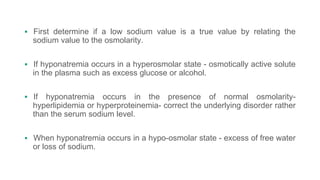
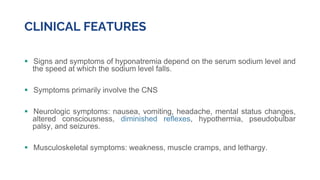
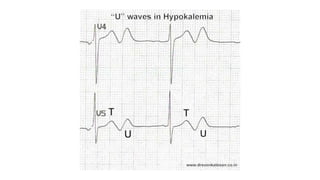
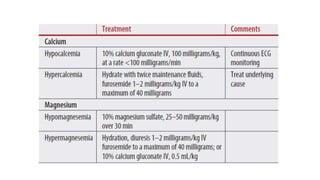
This document discusses fluid and electrolyte therapy in infants and children, focusing on dehydration causes, types, assessment, and treatment strategies. It emphasizes the importance of proper hydration methods, recognizing symptoms like weight loss, changes in mental status, and urine output, along with approaches for correcting electrolyte imbalances such as hyponatremia and hypernatremia. Additionally, it covers various conditions like hypokalemia, hypocalcemia, and hypermagnesemia, detailing their causes, clinical features, and treatment options.