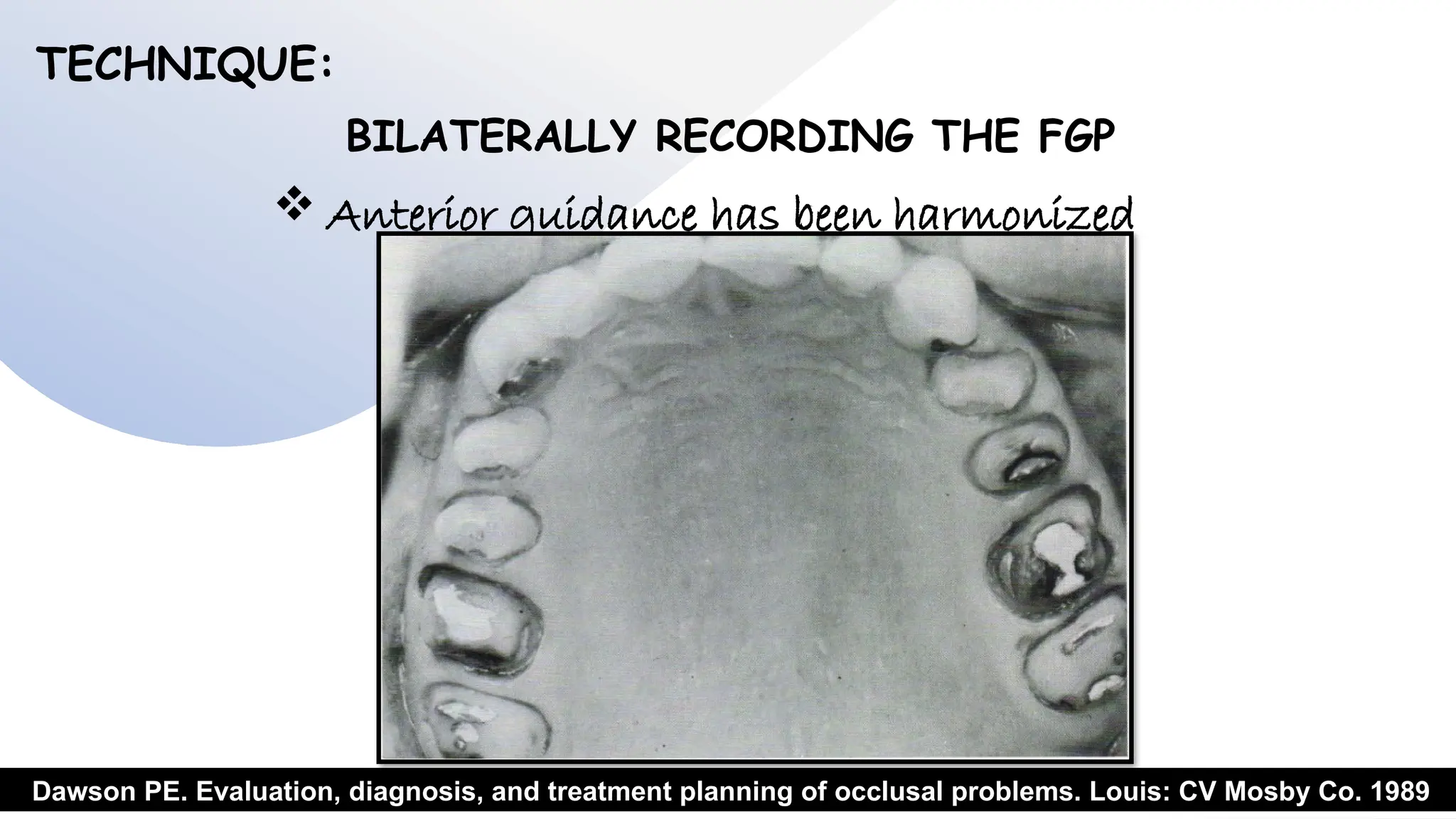
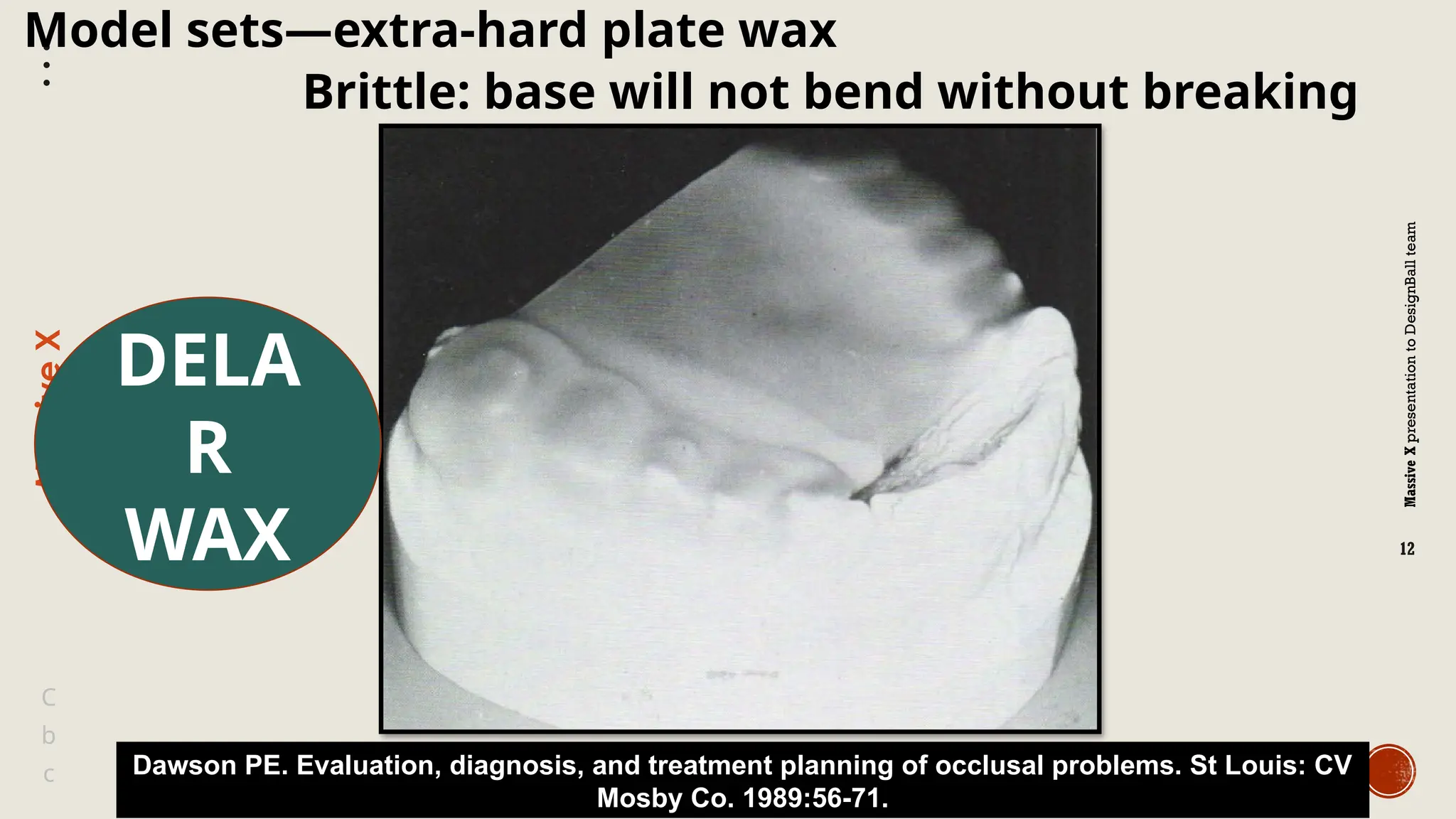
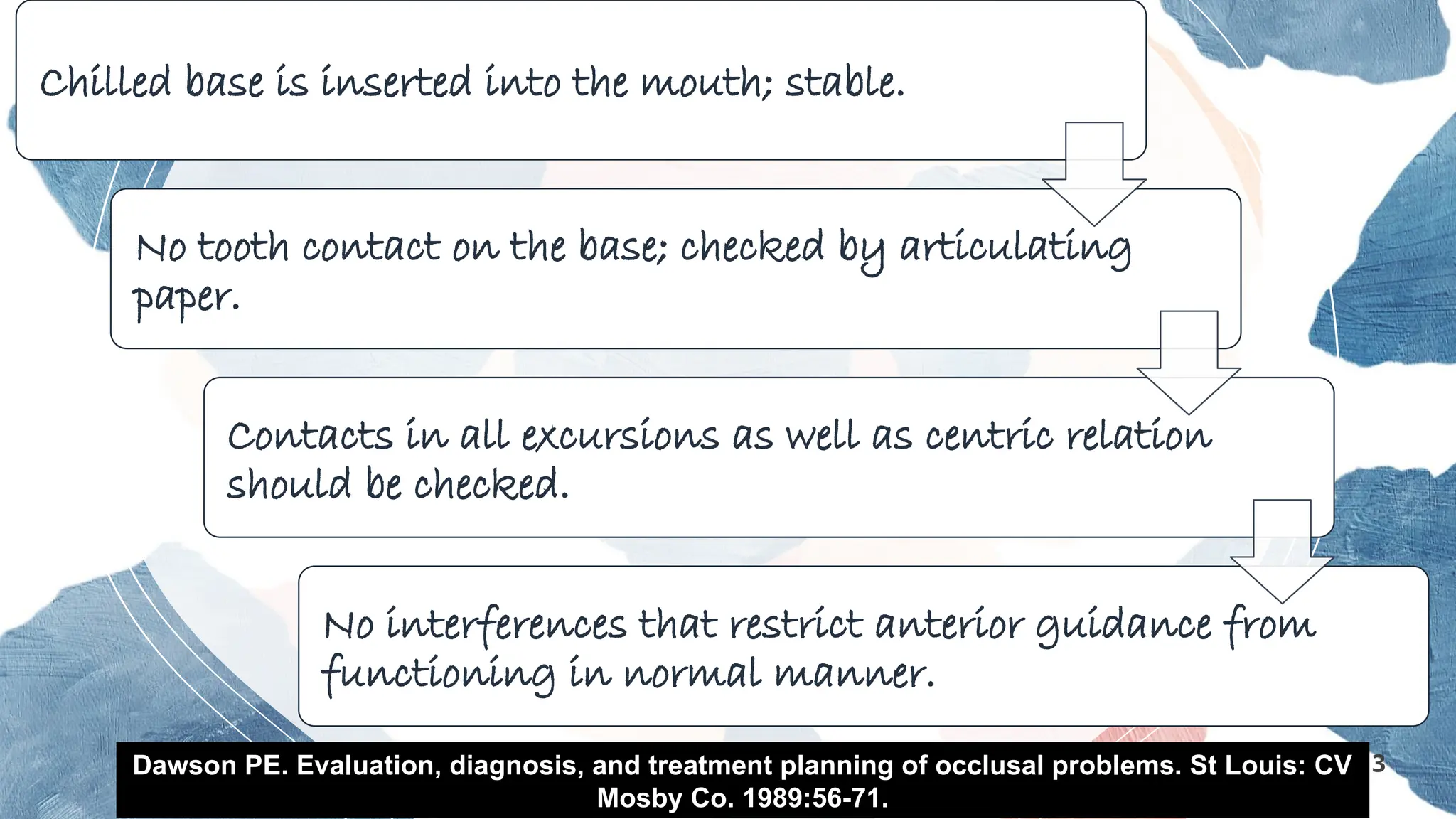
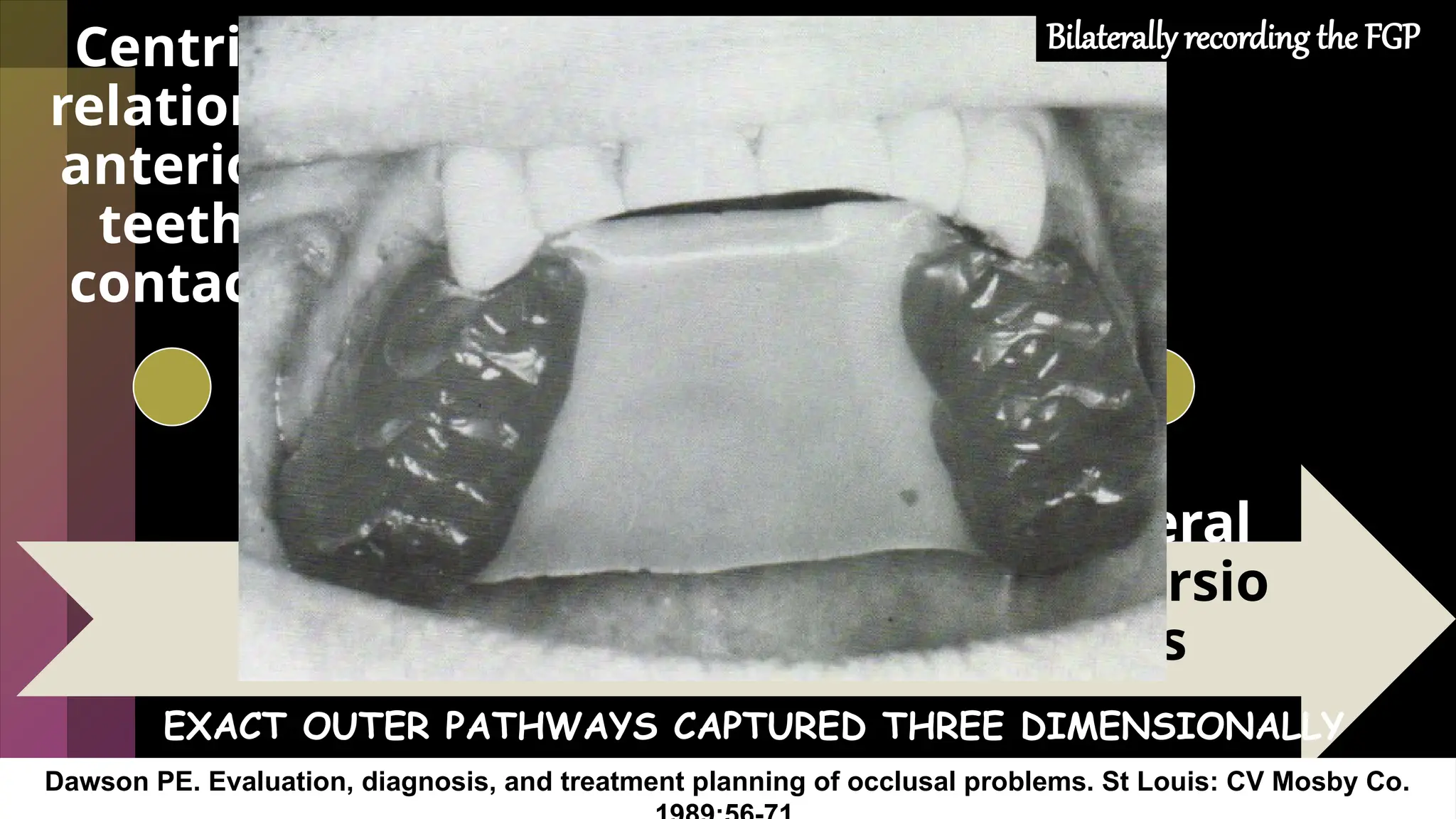
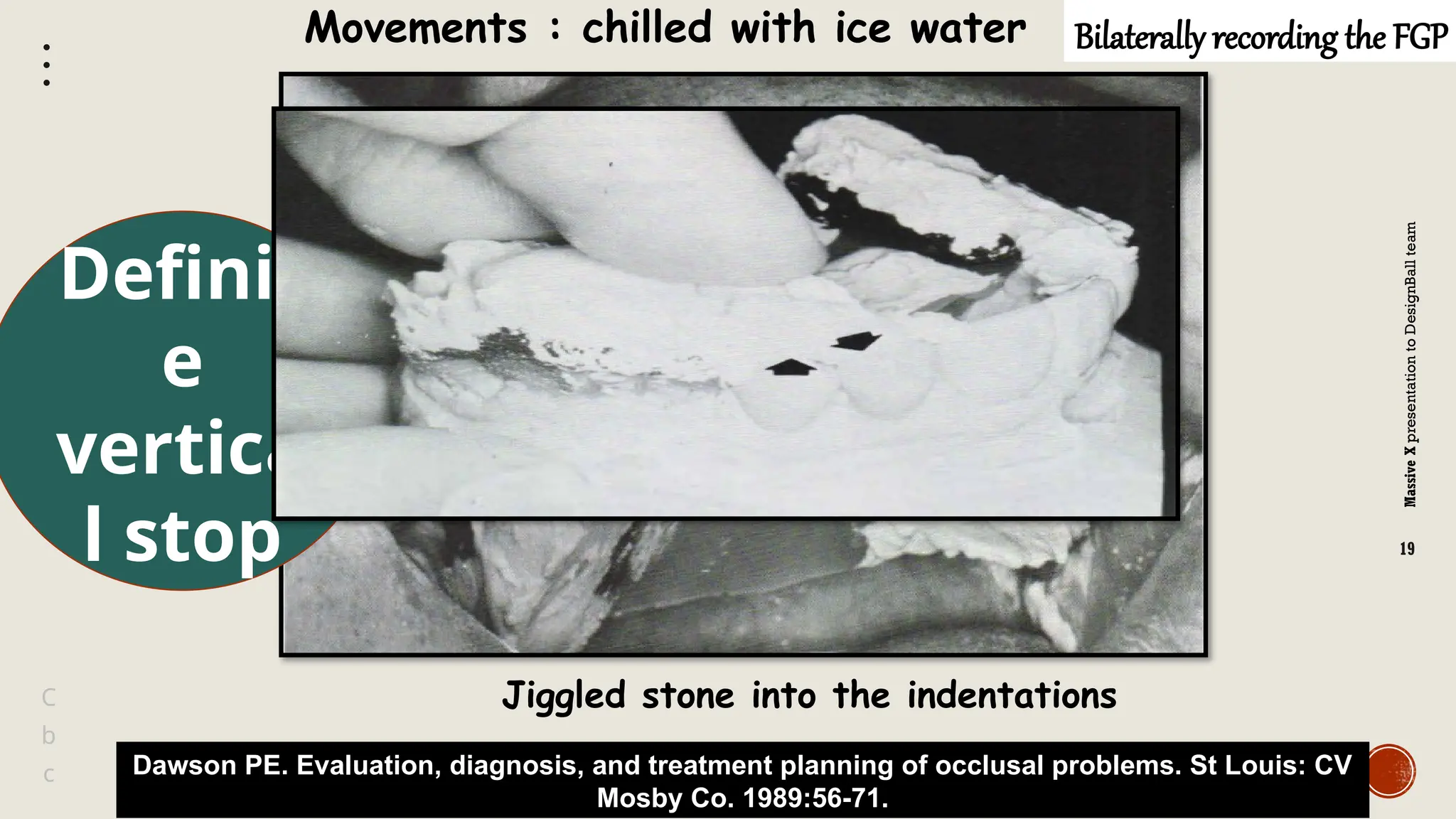
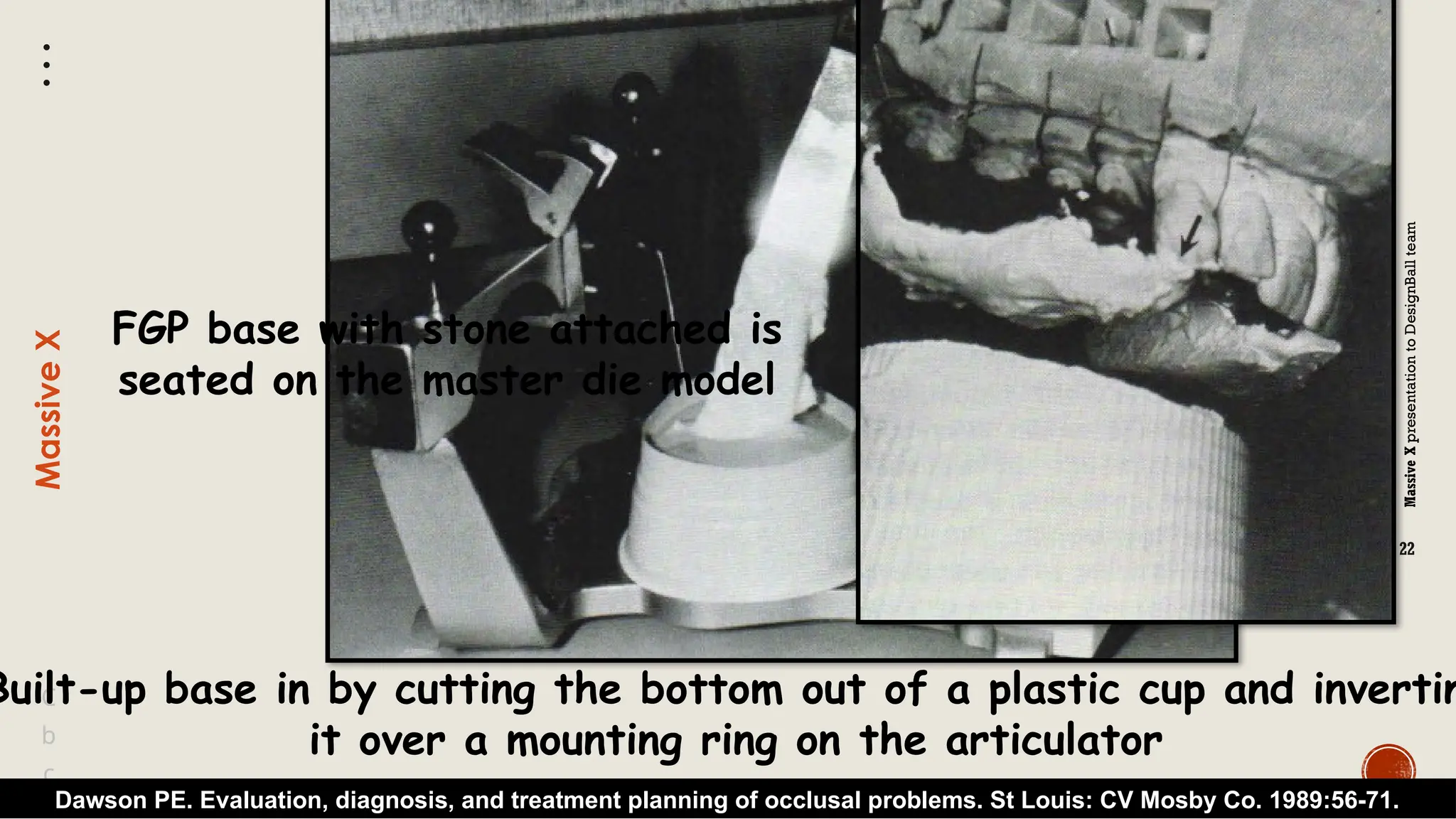
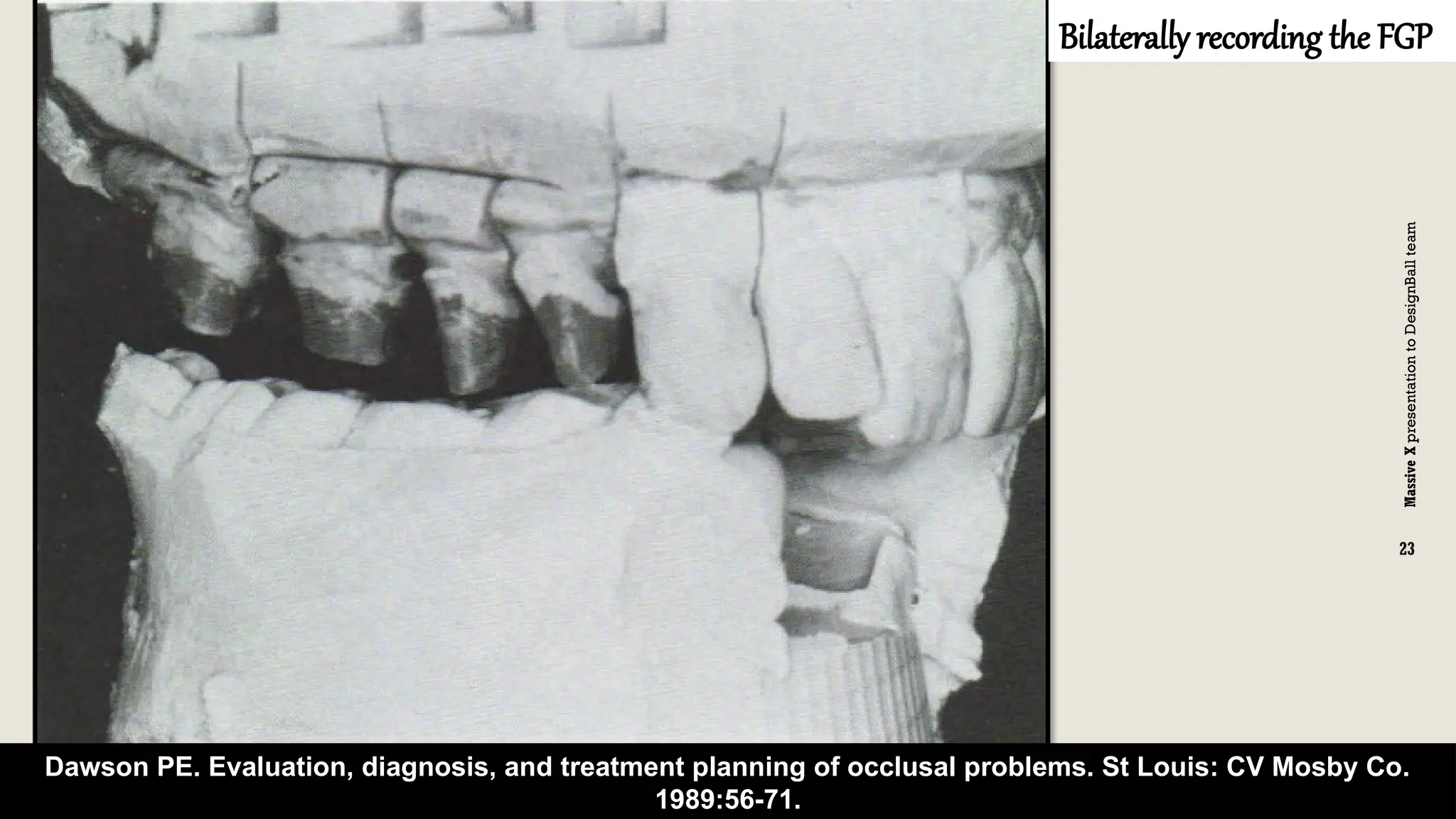
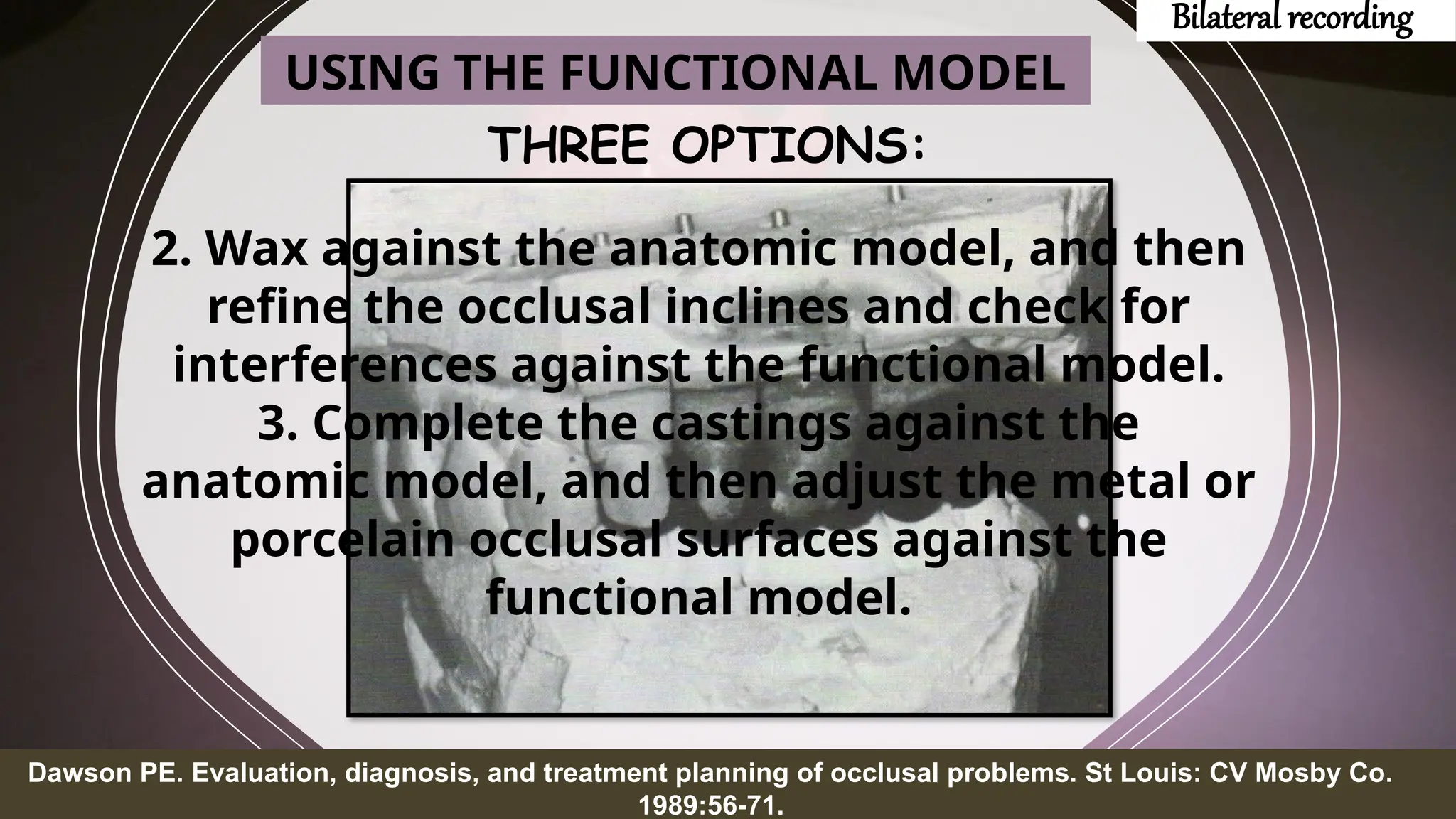
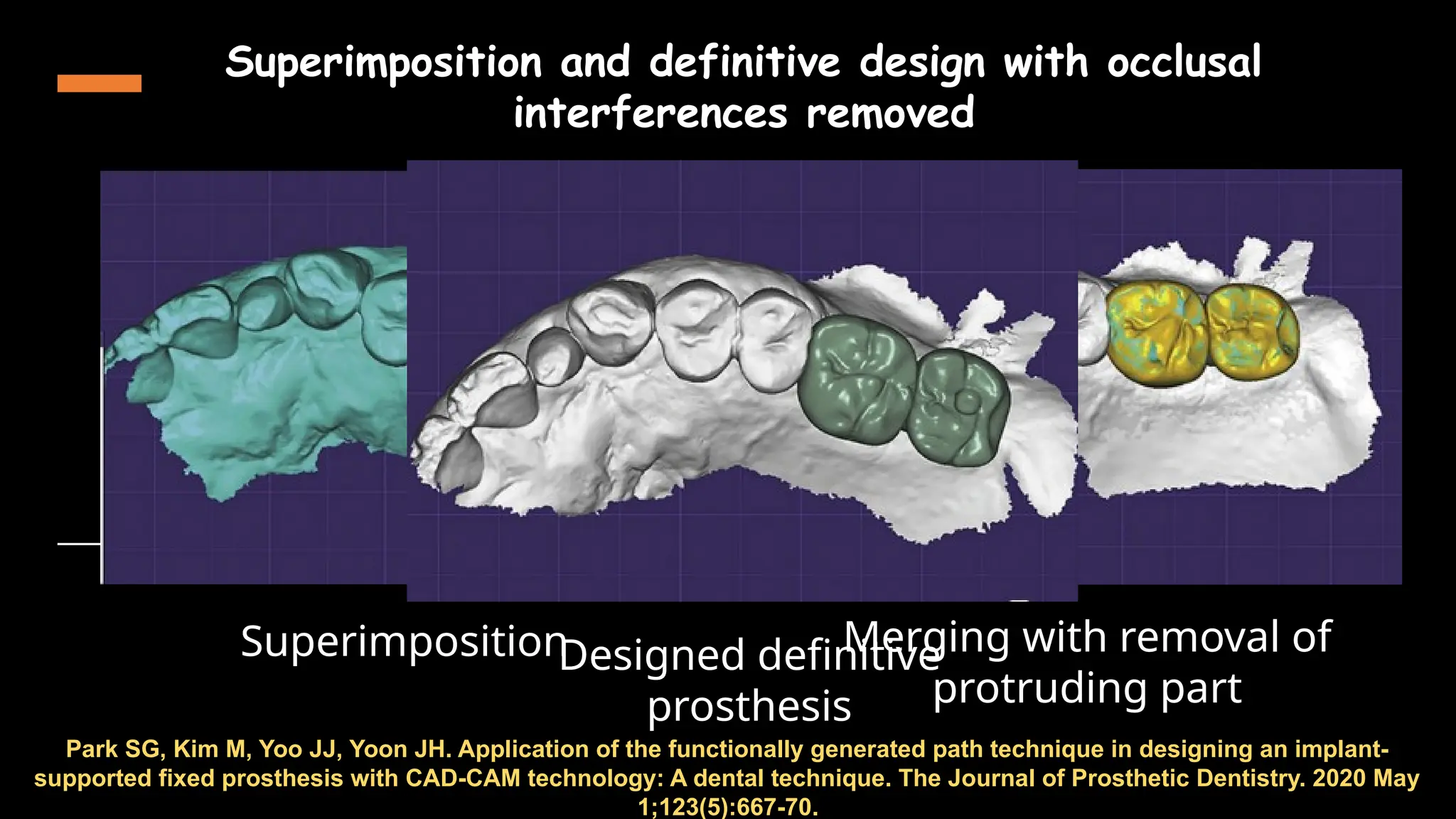
The document provides an overview of the functionally generated path (FGP) technique in dentistry, covering its introduction, historical background, uses, and techniques for different types of dental restorations. It emphasizes the importance of recording occlusal movements accurately and outlines procedures for achieving optimal occlusion in various clinical scenarios, such as single tooth restorations and quadrant dentistry. The conclusion highlights the relevance of FGP in improving dental rehabilitation outcomes.