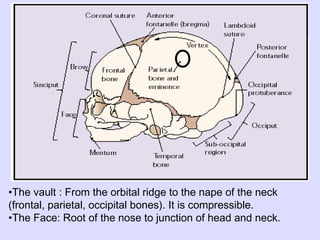
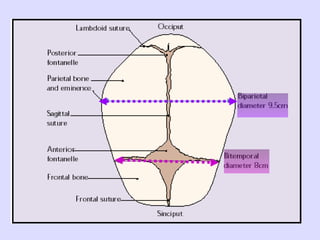
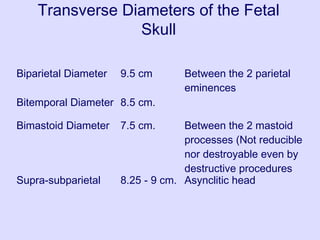
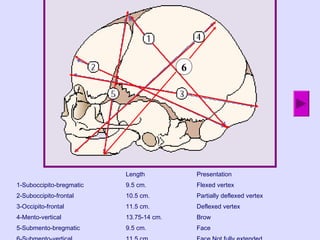
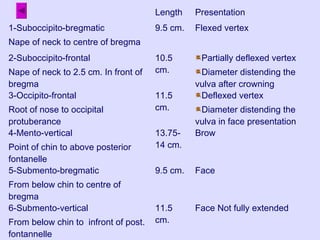
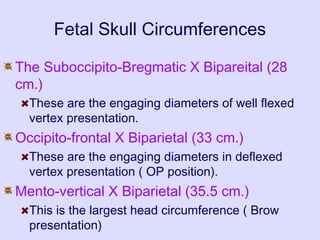
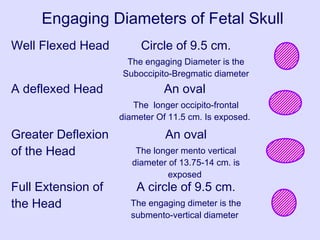
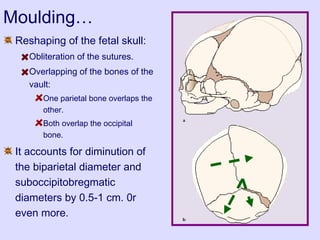
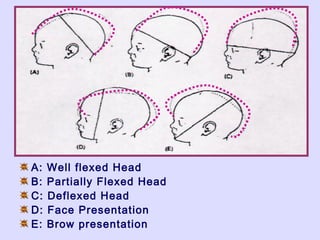
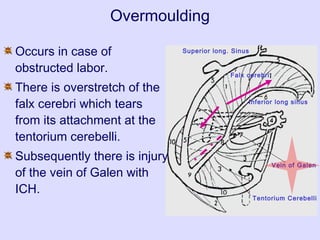
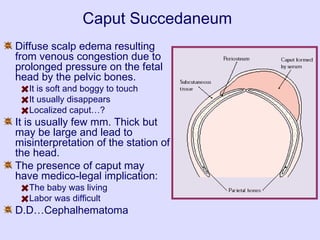
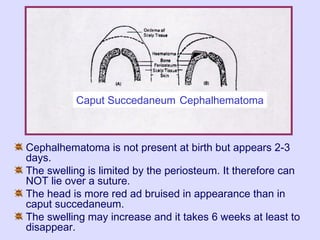
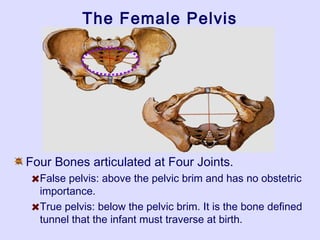
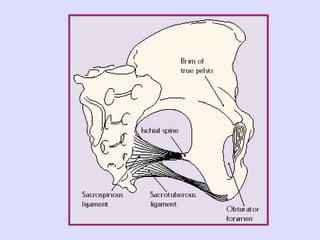
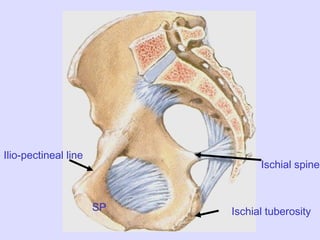
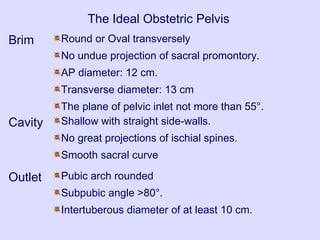
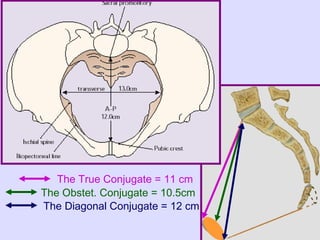
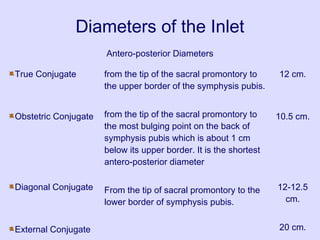
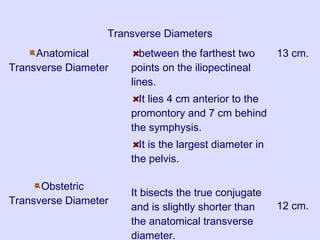
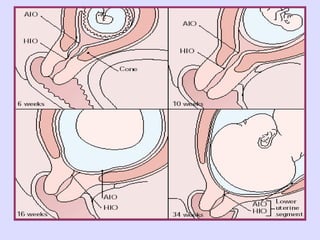
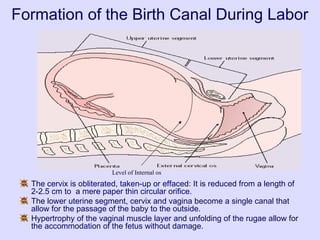
This document provides an overview of obstetric anatomy, including the fetal skull, pelvis, and soft tissues involved in childbirth. It describes the diameters and molding of the fetal skull, as well as caput succedaneum and cephalhematoma. It outlines the bones, joints, planes and diameters of the female pelvis and classifies the four pelvic types. It also discusses the formation of the lower uterine segment and birth canal during labor, the muscles of the pelvic floor, and episiotomy. In summary, it provides a detailed anatomical reference for the structures involved in fetal descent and passage through the birth canal.