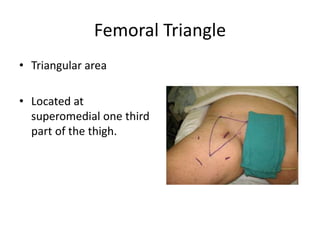
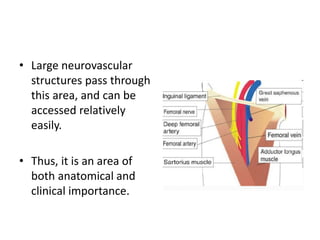
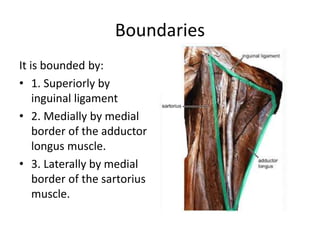
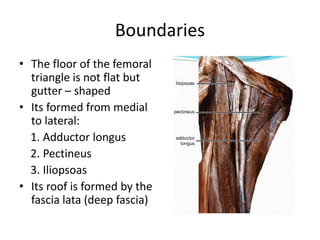
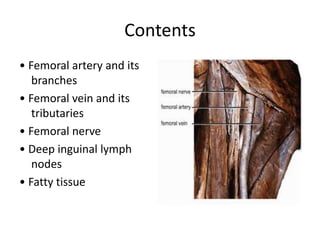
The femoral triangle is an anatomical region in the upper thigh bounded by the inguinal ligament, the adductor longus muscle, and the sartorius muscle. It contains the femoral artery, vein, and nerve. The femoral artery can be easily accessed in this region for procedures like coronary angiography. The femoral pulse can also be palpated here. Various structures like hernias, lymph nodes, and varicose veins may present clinically in the femoral triangle region.