FAT EMBOLISM SYNDROME: A MULTISYSTEM DISORDER
•Download as PPTX, PDF•
14 likes•1,976 views

Fat embolism syndrome is a serious complication of long bone fractures and other trauma involving bone marrow. Fat droplets released from the bone marrow can cause pulmonary and neurological dysfunction. While diagnosis is clinical, imaging may show a "snowstorm" pattern on chest x-ray or fat globules in blood viewed through a Swan-Ganz catheter. Treatment is supportive, focusing on oxygenation, ventilation, and prevention of deep vein thrombosis. Outcomes are often good if respiratory failure can be managed, though fulminant cases can be fatal. Prevention prioritizes early fracture stabilization to reduce intramedullary pressure.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to FAT EMBOLISM SYNDROME: A MULTISYSTEM DISORDER
Similar to FAT EMBOLISM SYNDROME: A MULTISYSTEM DISORDER (20)
Recently uploaded
Recently uploaded (20)
FAT EMBOLISM SYNDROME: A MULTISYSTEM DISORDER
- 1. FAT EMBOLISM SYNDROME DR. VASKAR HUMAGAIN RESIDENT, ORTHOPAEDICS AND TRAUMA SURGERY 2076/01/03
- 2. INTRODUCTION • Major cause of morbidity and mortality after fractures in the patient with multiple injuries. • It is a type of embolism in which the embolus consists of fatty material. • Embolus (Greek: plug) : detached intravascular solid, liquid, or gaseous mass that is carried by the blood to a site distant from its point of origin. • Fat embolism may be defined as a blockage of blood vessels by intravascular fat globules ranging from 10-40 µm in diameter • Fat embolism syndrome: It is a serious manifestation of fat embolism characterized by multisystem involvement (lungs are almost always involved) • Diagnosis of exclusion of other causes of dyspnea, hypoxia or confusion.
- 3. HISTORY • Zenker, a pathologist, 1st identified Fat Embolism syndrome at autopsy in 1862. • First diagnosed in 1873 by Dr. Von Bergmann • Fenger and Salisbury, In 1879 , first described this syndrome in American Literature.
- 4. ETIOLOGY Related to Trauma • Long bone ( Femur, Tibia ) fracture • Pelvic fractures • Orthopaedic procedures (intramedullary reaming, hip and knee arthroplasty) • Soft tissue injuries (eg chest compression with or without rib fractures) • Burns • Liposuction • Bone marrow harvesting and transplant • Bone Marrow biopsy
- 5. ETIOLOGY - ATRAUMATIC A. Disease related: • Diabetes, Pancreatitis, Osteomyelitis, Sickle cell haemoglobinopathies , burns, SLE, panniculitis B. Drug related: • Steroid therapy, Lipid infusion, Cyclosporine A solvent
- 6. EPIDEMIOLOGY • Incidence ranges from <1% to 29% in different studies • Fat globules detected in blood of 67% of orthopaedic trauma patients. Increased to 95% in blood samples near to the fracture site • The presence of fat globules in the blood does not automatically lead to FES. • Men are more likely than women. Rare in children aged 0-9 years. Age group commonly affected 10- 39 years
- 7. PATHOPHYSIOLOGY • The pathophysiology of the fat embolism is not clearly established • Mechanical Hypothesis (Obstruction of Vessels and Capillaries) • Biochemical Hypothesis (Toxicity of Free Fatty Acids) • Coagulation Theory
- 8. Mechanical Hypothesis (Gauss,1924) • mechanical obstruction of the systemic vasculature by fat droplets released from the bone marrow of damaged bone due to high intramedullary pressure during elective orthopedic surgery or trauma, travels through torn veins and lodges in distal capillaries causing mechanical obstruction. • Smaller fat droplets travel through the pulmonary capillaries into the systemic circulation: Embolization to cerebral vessels or renal vessels also leads to central nervous system and renal dysfunction
- 9. Biochemical Hypothesis • FES is dependent upon degradation of the embolized fat into free fatty acids. • Neutral fat does not cause an acute lung injury, it is hydrolyzed over the course of hours to several products, including FFA, which cause ARDS in animal models. • CRP (acute phase reactant), which is elevated in trauma patients, appears to be responsible in lipid agglutination (FES) for both traumatic and non- traumatic FES. Lehmann and Moore, 1927
- 10. Coagulation Theory • This states that tissue thromboplastin is released with marrow elements following long bone fractures . • This activates the complement system and extrinsic coagulation cascade via direct activation of factor VII . • These lead to increase pulmonary vascular permeability, both by their direct actions on the endothelial lining and through the release of numerous vasoactive substances.
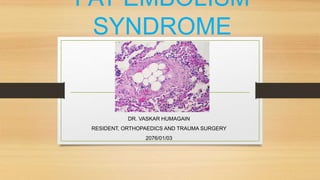
- 12. An Oil Red O stain demonstrates the fat globules within the pulmonary arterioles. The globules stain reddish-orange.
- 13. ↑ in intra medullary pressure → fat droplets → get filtered in the pulmonary circulation minute droplets go through pulmonary circulation & get trapped in cerebral circulation alveolar lipase → hydrolysis of fat → release of fatty acids (palmitic, stearic, oleic acids) Neutralisation by albumin failure of neutralisation by albumin ->> fatty acids + calcium → intercellular septa rupture → diffuse areas of haemorrhage & oedema in pulmonary interstitium & alveolar space Integrins CD11b & CD18 cause adherence of neutrophils & endothelium Injured pneumocytes stop surfactant production → collapse of alveoli
- 14. Clinical Features • Diagnosis is made CLINICALLY NOT CHEMICALLY. • It does not matter how much fat globules are in the circulation, it just matters if you have their side effects. • FES typically manifests 24 to 72 hours after the initial insult. Rarely <12 hrs or >72 hrs.
- 15. Early Signs • Dyspnea • Tachypnea • Hypoxemia Respiratory manifestations in 95% of the cases Drowsiness with oliguria is almost pathognomonic
- 16. CNS Manifestations: • from mild headache to significant cerebral dysfunction (restlessness, disorientation, confusion, seizures, stupor or coma) • Fortunately, almost all neurological deficits are transient and fully reversible.
- 17. Rash • Petechial rash on upper anterior trunk, arm and neck, buccal mucosa & conjunctivae , may be transient • Results from occlusion of dermal capillaries by fat globules and then extravasations of RBC • PATHOGNOMONIC, but only present in 20-50% of patients.
- 19. Renal Manifestations • Oliguria • haematuria • anuria
- 20. Ocular Manifestations • On fundoscopy, Purtscher’s retinopathy may be seen • Cotton wool exudates, macular oedema and macular haemorrhage can also be found.
- 21. CVS Involvement • Early persistent tachycardia, though nonspecific, is almost invariably present in all patients with fat embolism
- 22. Systemic Fever • Moderate fever with a disproportionately high pulse rate is a very common early sign
- 23. Gurd’s and Wilson’s criteria Major Criteria • Petechial rash • Respiratory insufficiency • Cerebral involvement Minor Criteria • Tachycardia • Fever • Retinal changes • Jaundice • Renal signs • Thrombocytopenia • Anaemia • High Erythrocyte Sedimentation Rate • Fat macroglobulinemia
- 24. Lindeque’s criteria (FES = femur fracture +/- tibia fracture + 1 feature) Based on respiratory parameters 1. Sustained PaO2 of < 8 kPa (60mm Hg) 2. Sustained PaCO2 of >7.3 kPa (55mm Hg) or a pH <7.3 3. Sustained respiratory rate >35 breaths/min, despite sedation 4. Increased work of breathing: dyspnoea, accessory muscle use, tachycardia, and anxiety
- 26. Sevitt’s Classification (1962) • Subclinical • Non-fulminant • Fulminant
- 27. Sub-clinical FES • Around 3 days post trauma • Probably occurs in almost all long bone fractures of the lower extremity and fractures of the pelvis • Characterised by decreased PaO2, decreased Hb% and decreased platelets. No clinical signs and symptoms of respiratory insufficiency.
- 28. Non-fulminant FES • Any time ,up to 6 days post trauma • Clinical signs and symptoms are clearly evident. • Petechiae, tachycardia, respiratory failure, and signs of CNS embolism. Thrombocytopaenia, anaemia, and coagulation abnormalities can be found, as can pulmonary alveolar and interstitial opacities on chest x ray
- 29. Fulminant FES • Occurs very suddenly and rapidly after injury, and progresses very quickly, often resulting in death within a few hours of the initial trauma. Clinical features are acute respiratory failure, acute cor pulmonale and embolic neurological changes. • These occur shortly after injury and often result in the death of the patient.
- 30. Investigations • Hematology and Biochemistry • Urine and Sputum • Radiological
- 31. Hematological Investigations • An unexplained anemia (70% of patients) and thrombocytopenia (platelet count <1,50,000 /mm3 in up to 50% of patients) are often found. • Hypocalcemia (due to binding of free fatty acids to calcium) and elevated serum lipase have also been reported. • Hypofibrinogenemia, raised ESR and prolongation of prothrombin time may be seen • ABG reveals a low partial pressure of O2 and low partial pressure of CO2 with respiratory Alkalosis
- 32. Urine and sputum • Analysis of the sputum or urine for fat has not proved to be accurate. • Bronchoalveolar lavage and staining with Oil Red O can demonstrate neutral fat. Microscopic examination of the blood for fat globules when it is collected from pulmonary circulation through Swan-Ganz catheter is the diagnostic test.
- 33. Radiological • CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral infiltrates , enlargement of right side of the heart. • CT chest: ground glass opacification with interlobular septal thickening • CT Head: general edema, usually nonspecific • MRI brain: Low density on T1, and high intensity T2 signal, correlates to degree of impairment • Diffusion weighted-MRI (DW-MRI) of the brain showing a “Star Field” pattern of multiple small high-intensity lesions with diffusion restriction supports the diagnosis.
- 34. Differential Diagnosis • Pulmonary Embolism • Thrombotic thrombocytopenic purpura
- 36. Management • There is no specific therapy for the fat embolism syndrome, so prevention, early diagnosis, and adequate symptomatic treatment are of paramount importance • Adequate oxygenation and ventilation • Stable hemodynamics • Blood products as clinically indicated • Hydration / i.v. fluids • Prophylaxis of deep venous thrombosis and stress related gastrointestinal bleeding
- 37. Management • Nutritional support • Corticosteroids • Heparin • Antibiotics • Early immobilisation of the fracture decreases the incidence of FES
- 38. Prevention • Because treatment is primarily supportive, our focus must be on prevention. • In trauma, early fracture stabilization decreases the rate of FE syndrome. • Use of RIA • In arthroplasty, computer navigation and alternative cementation techniques decrease fat embolization,
- 39. Measures to decrease the chances of fat embolism while reaming • Use of sharp reamer • Decreasing RPM while reaming • Gradually increasing the size of reamer by 0.5 mm • RIA technique • Use of flexible reamer • Not fixing B/L femur fracture at the same setting
- 40. Summary • Fat embolism occurs in many traumatic and atraumatic conditions and is largely asymptomatic. Preventative measures include early immobilization of fractures and methods to reduce intramedullary pressure during surgical manoeuvres. Treatment is largely symptomatic with therapy for respiratory failure similar to that used in management of acute respiratory distress syndrome
- 41. References 1. Apley’s and Solomon’s System of Orthopaedics and Trauma, 10th Edition, CRC Press, Taylor and Francis Group 2. Essential Orthopaedics Principles and Practice, Manish Kumar Varshney, Jaypee Publishers 3. Textbook of Orthopaedics and Trauma, Second Edition, GS Kulkarni, Jaypee Publishers 4. Fat emboli syndrome and the orthopaedic trauma surgeon: lessons learned and clinical recommendations. Dunn, R.H., Jackson, T., Burlew, C.C. et al. International Orthopaedics (SICOT) (2017) 41: 1729. https://doi.org/10.1007/s00264-017-3507-1 5. Rothberg DL, Makarewich CA. Fat Embolism and Fat Embolism Syndrome. J Am Acad Orthop Surg. 2019 Apr 15;27(8):e346-e355. doi: 10.5435/JAAOS-D-17-00571. 6. Bollineni VR, Gelin G, Van Cauter S. Cerebral Fat Embolism Syndrome. J Belg Soc Radiol. 2019 Apr 2;103(1):20. doi: 10.5334/jbsr.1781.
- 42. THANK YOU
Editor's Notes
- this theory is animal model based and circumstantial at best.
- this theory is animal model based and circumstantial at best.
- Seen here with Oil red O stain in a peripheral cerebral artery branch are globules of lipid. This is fat embolism syndrome.
- Stabilize cell membrane, ↓ PMN adhesion, prevent surfactant reduction, protect capillary endothelium, activation and minimize transudation