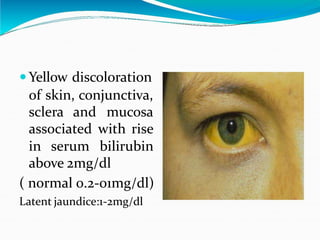
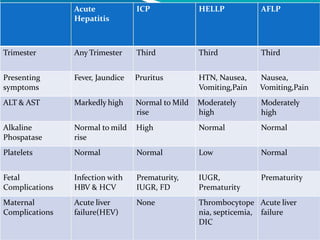
This document discusses jaundice in pregnancy. It begins by defining jaundice and describing the physiological changes that occur in the liver during pregnancy, including increases in certain enzymes and proteins. It then examines various causes of jaundice in pregnancy, such as acute fatty liver disease, intrahepatic cholestasis, preeclampsia/HELLP syndrome, viral hepatitis, and others. For each condition, it provides details on pathogenesis, clinical presentation, diagnosis, management, and prognosis. Throughout, it emphasizes the importance of prompt delivery in treating many pregnancy-related liver conditions.