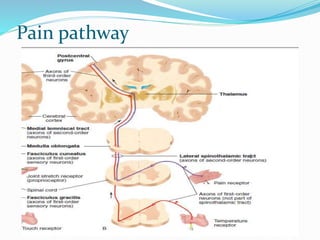
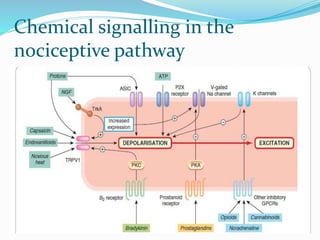
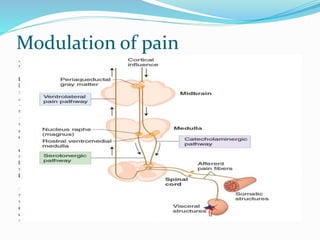
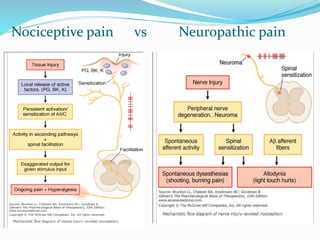
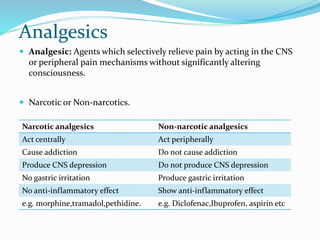
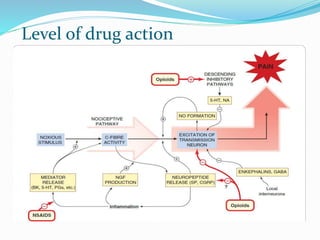
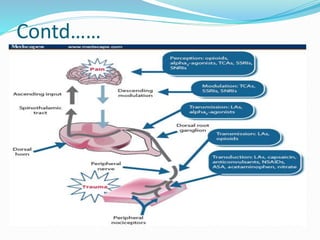
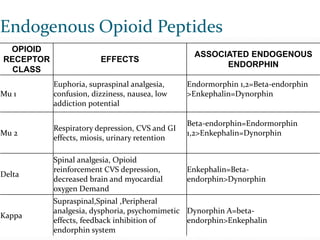
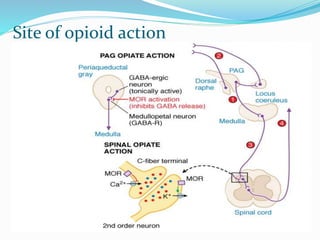
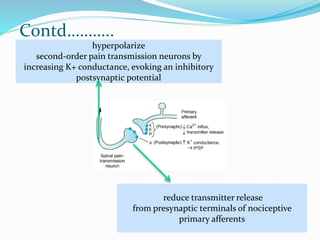
This document summarizes pain physiology and the evaluation of analgesics. It discusses the definition of pain, pain pathways, endogenous opioid peptides, and types of analgesics. Methods for evaluating analgesics include in vitro tests like receptor binding assays and in vivo tests using various pain models in animals. Acute pain models include thermal, electrical, chemical and mechanical stimuli. Chronic pain models examine neuropathic pain and cancer pain. While no single model perfectly mimics human pain, animal models remain important for assessing analgesic drug activity.