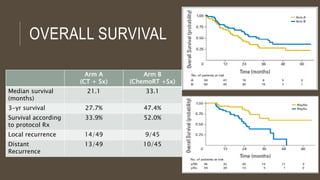
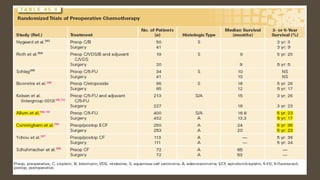
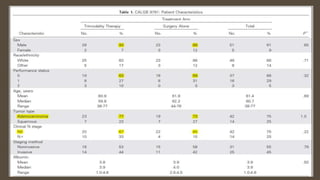
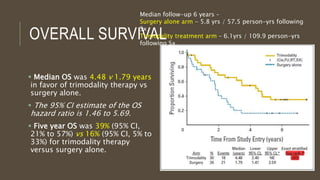
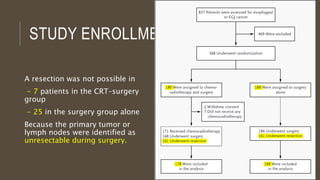
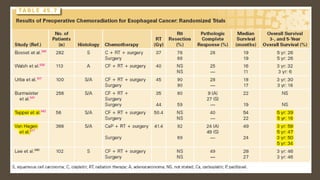
This document discusses several landmark trials comparing different treatment approaches for esophageal cancer. The CALGB 9781 trial compared trimodality therapy (chemotherapy, radiation therapy, and surgery) to surgery alone and found improved overall survival and progression-free survival with trimodality therapy. Median overall survival was 4.48 years with trimodality therapy versus 1.79 years with surgery alone. The trial was closed early due to poor accrual, resulting in a small sample size.

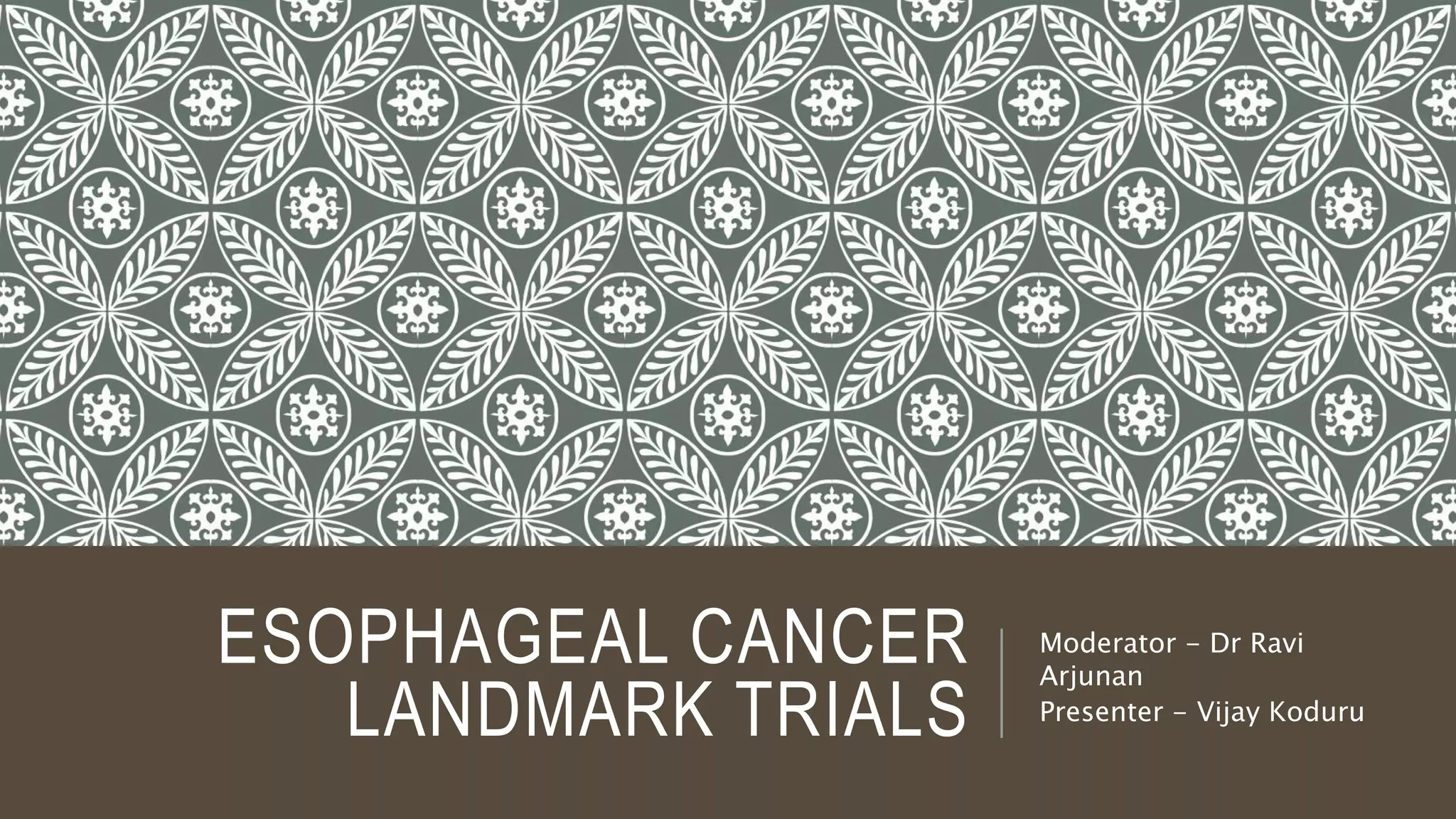
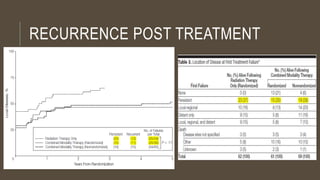
![OVERALL SURVIVAL
By 5 years,
26% (95% confidence
interval [CI], 15%-37%) of
the randomized combined
modality group
14% (95% CI, 6%-23%) of
the nonrandomized
combined modality group
were alive
NONE in the RT group.](https://image.slidesharecdn.com/journalclubesophagealtrials-180831171147/85/Esophageal-carcinoma-trials-12-320.jpg)

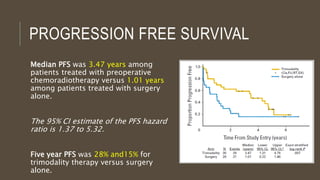

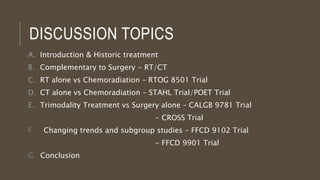
![OVERALL
SURVIVAL
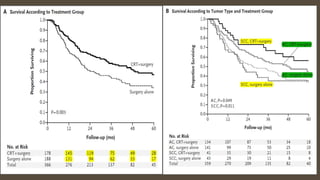
48.6 months (95% CI 32.1–65.1) in
the neoadjuvant CTRT plus surgery
group
24.0 months (14.2–33.7) in the
surgery alone group (HR 0.68 [95% CI
0.53–0.88])](https://image.slidesharecdn.com/journalclubesophagealtrials-180831171147/85/Esophageal-carcinoma-trials-73-320.jpg)
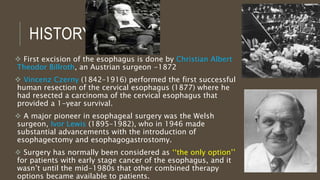
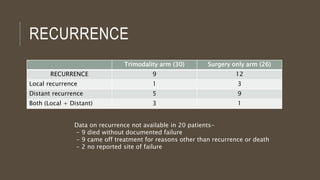
![OVERALL
SURVIVAL
SCC
81.6 months (95% ci 47.2–116.0) in the
neoadjuvant CTRT plus surgery group
21.1 months (15.4–26.7) in the surgery
alone group (HR 0.48 [95% CI 0.28–
0.83])
Adenocarcinoma
43.2 months (24.9–61.4) in the
neoadjuvant CTRT plus surgery group
27.1 months (13.0–41.2) in the surgery
alone group (HR 0.73 [95% CI 0.55–0.98](https://image.slidesharecdn.com/journalclubesophagealtrials-180831171147/85/Esophageal-carcinoma-trials-74-320.jpg)
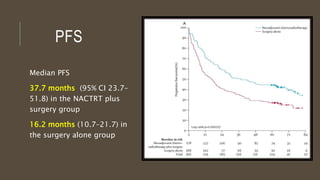
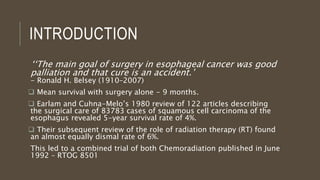
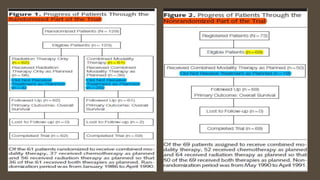
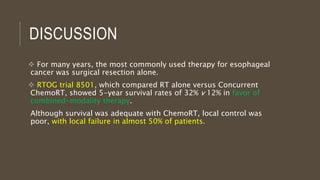
![PFS
SCC
74.7 months (95% CI 55.1–94.4) in
the NACTRT plus surgery group
11.6 months (4.4–18.8) in the
surgery alone group (HR 0.48 [95%
CI 0.28–0.82]
ADENOCARCINOMA
29.9 months (95% CI 15.9–43.9) in
the NACT plus surgery group
17.7 months (11.9-23.5) in the
surgery alone group (HR 0.69[95%
CI 0.52–0.9]](https://image.slidesharecdn.com/journalclubesophagealtrials-180831171147/85/Esophageal-carcinoma-trials-76-320.jpg)
























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)














