Downloaded 1,944 times







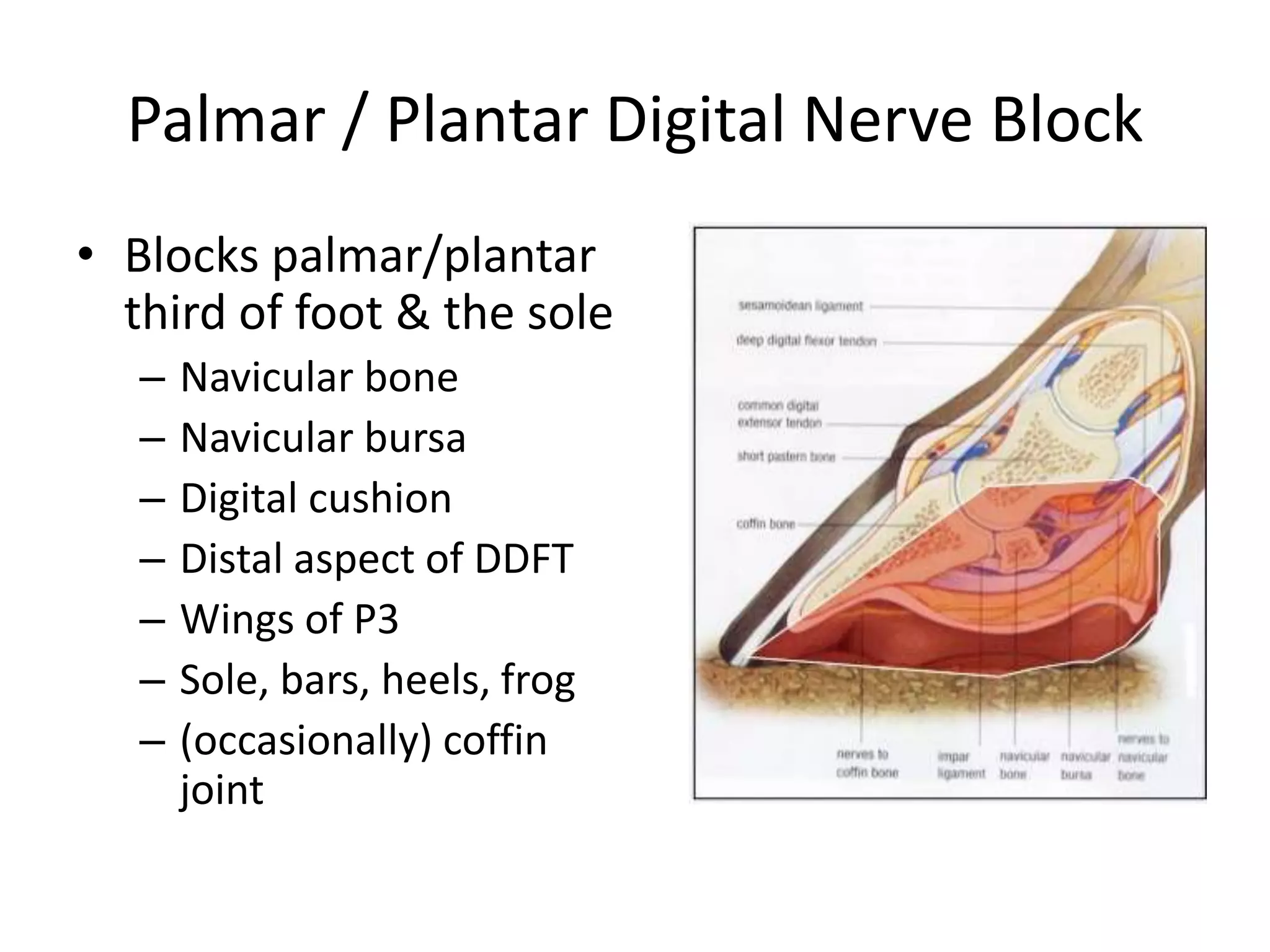
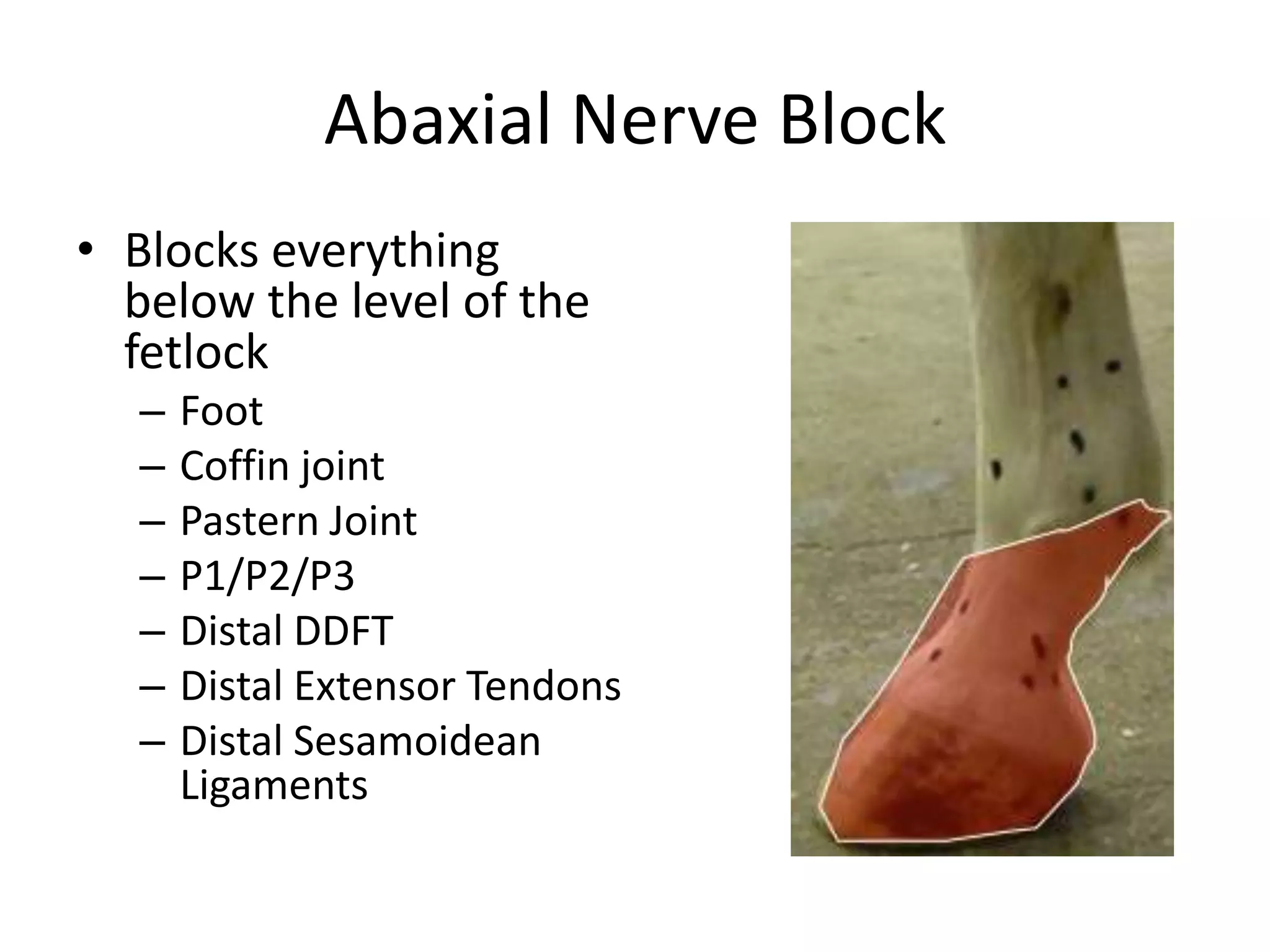

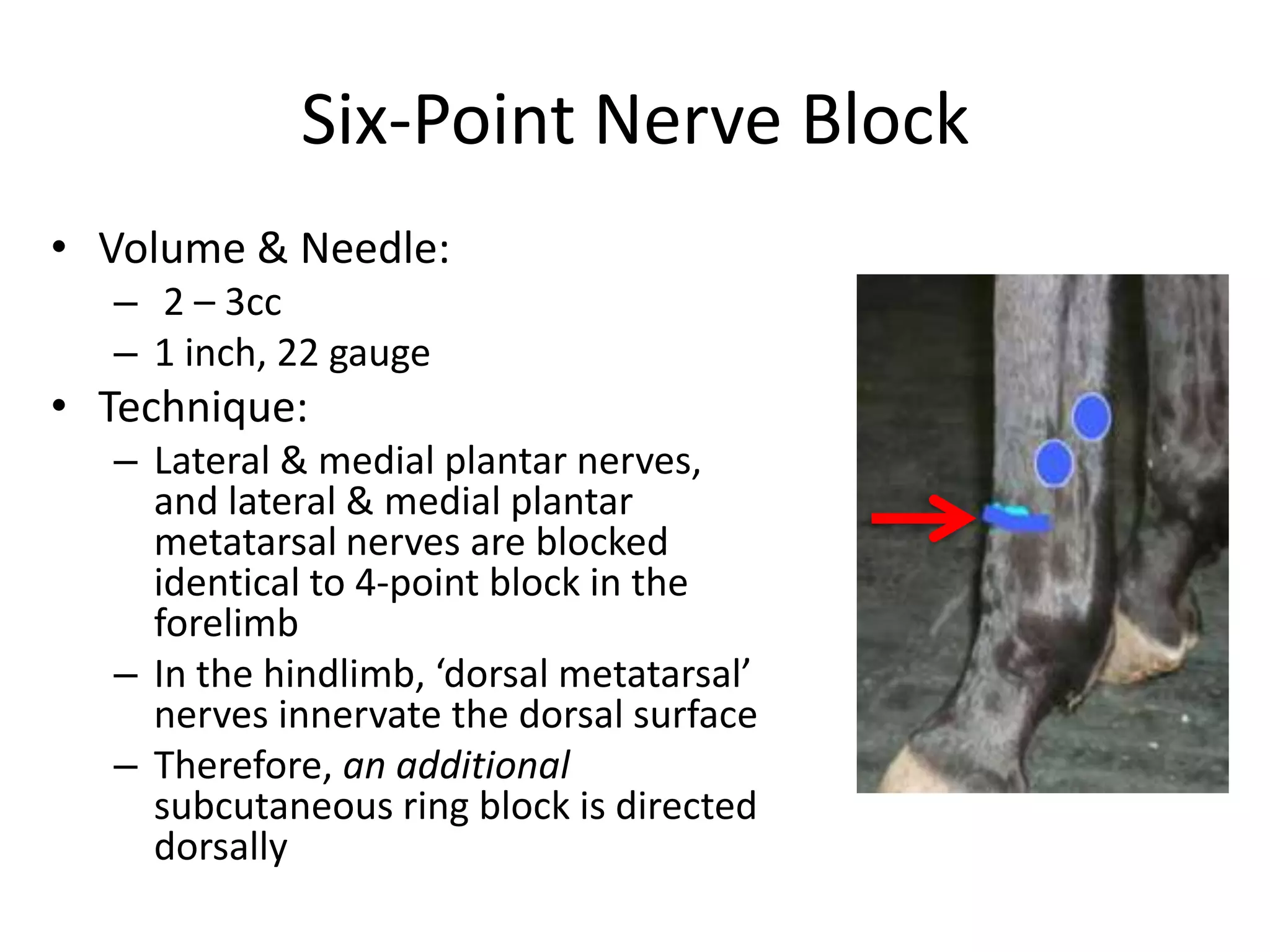









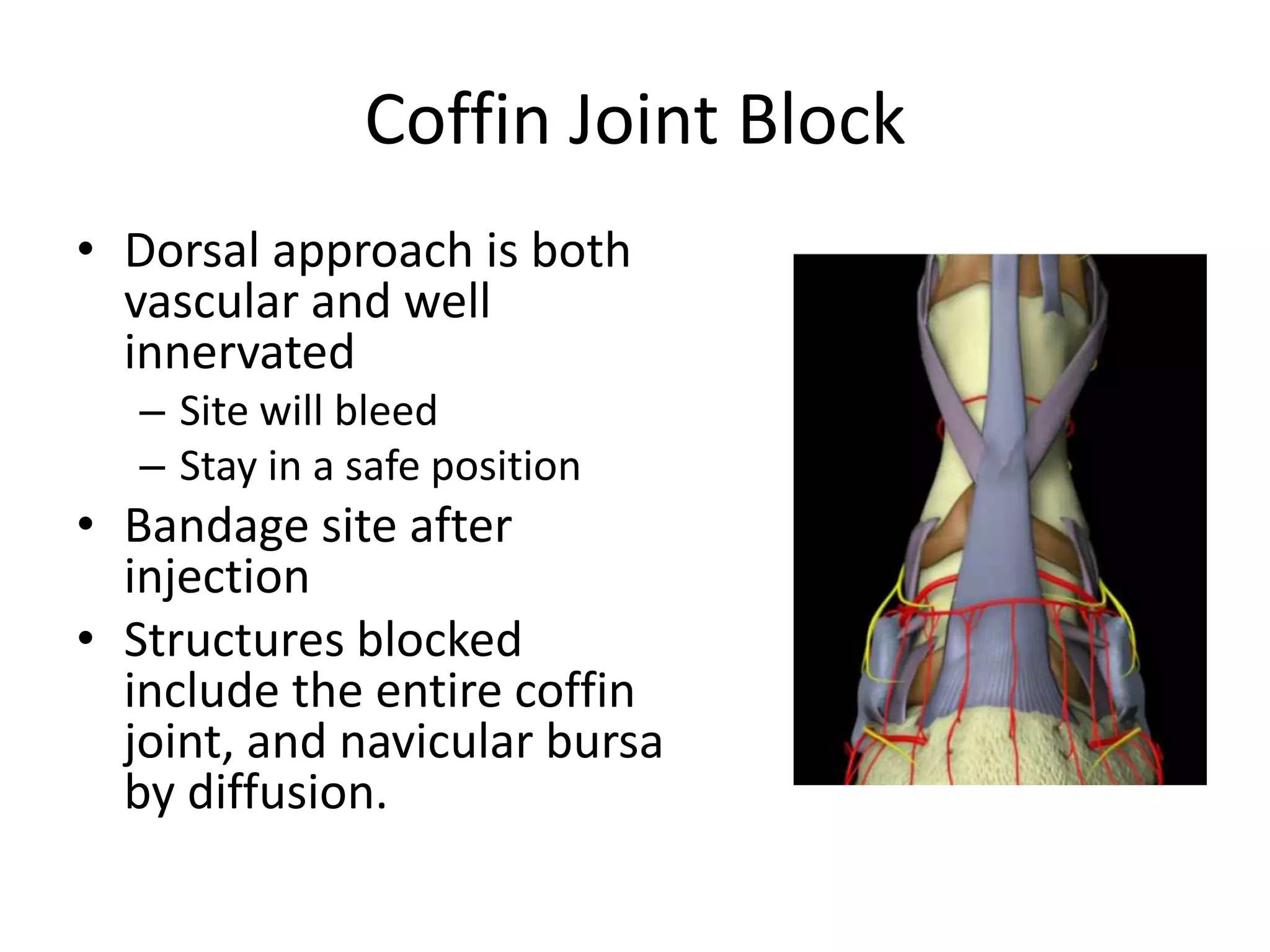

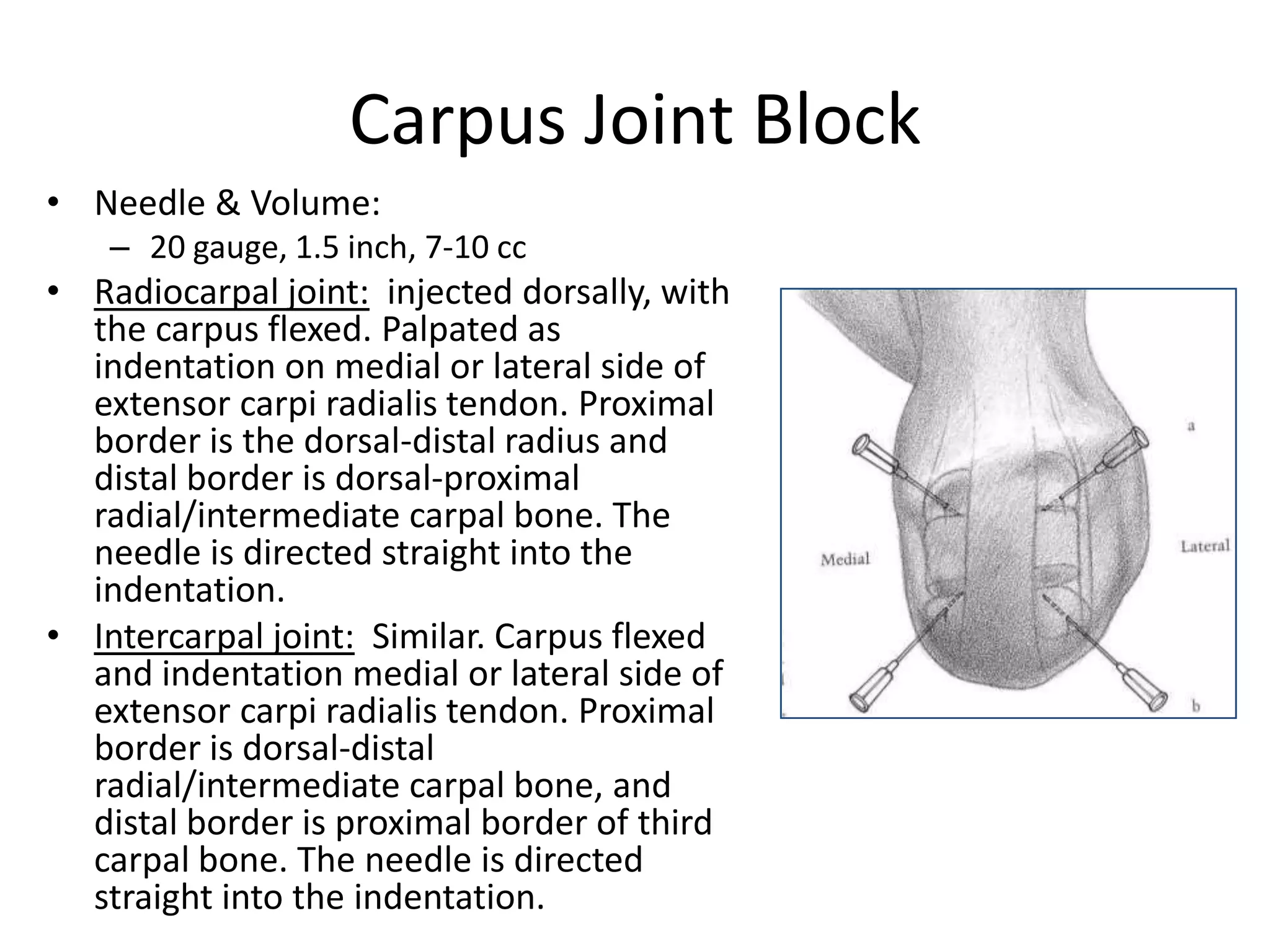



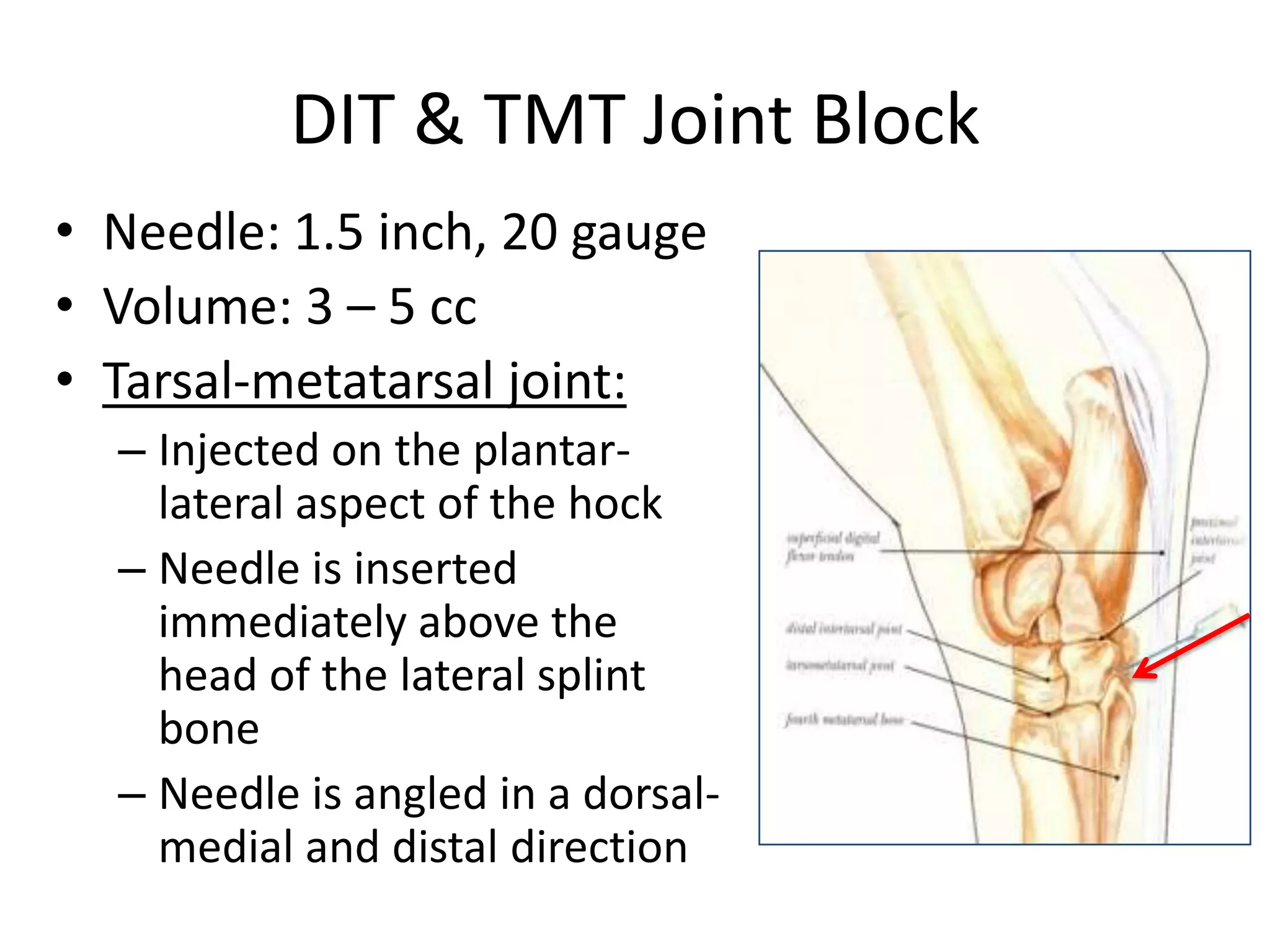
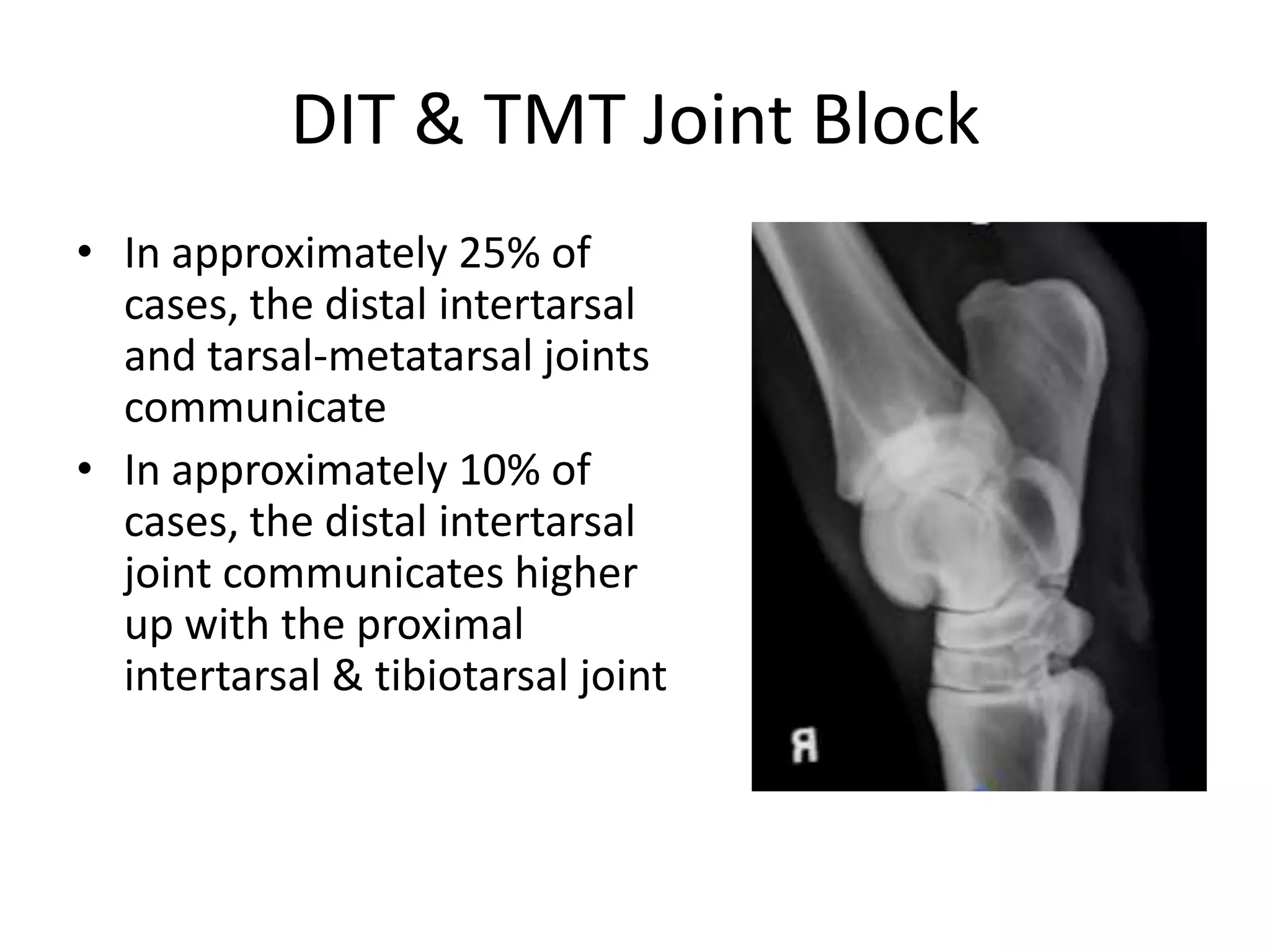


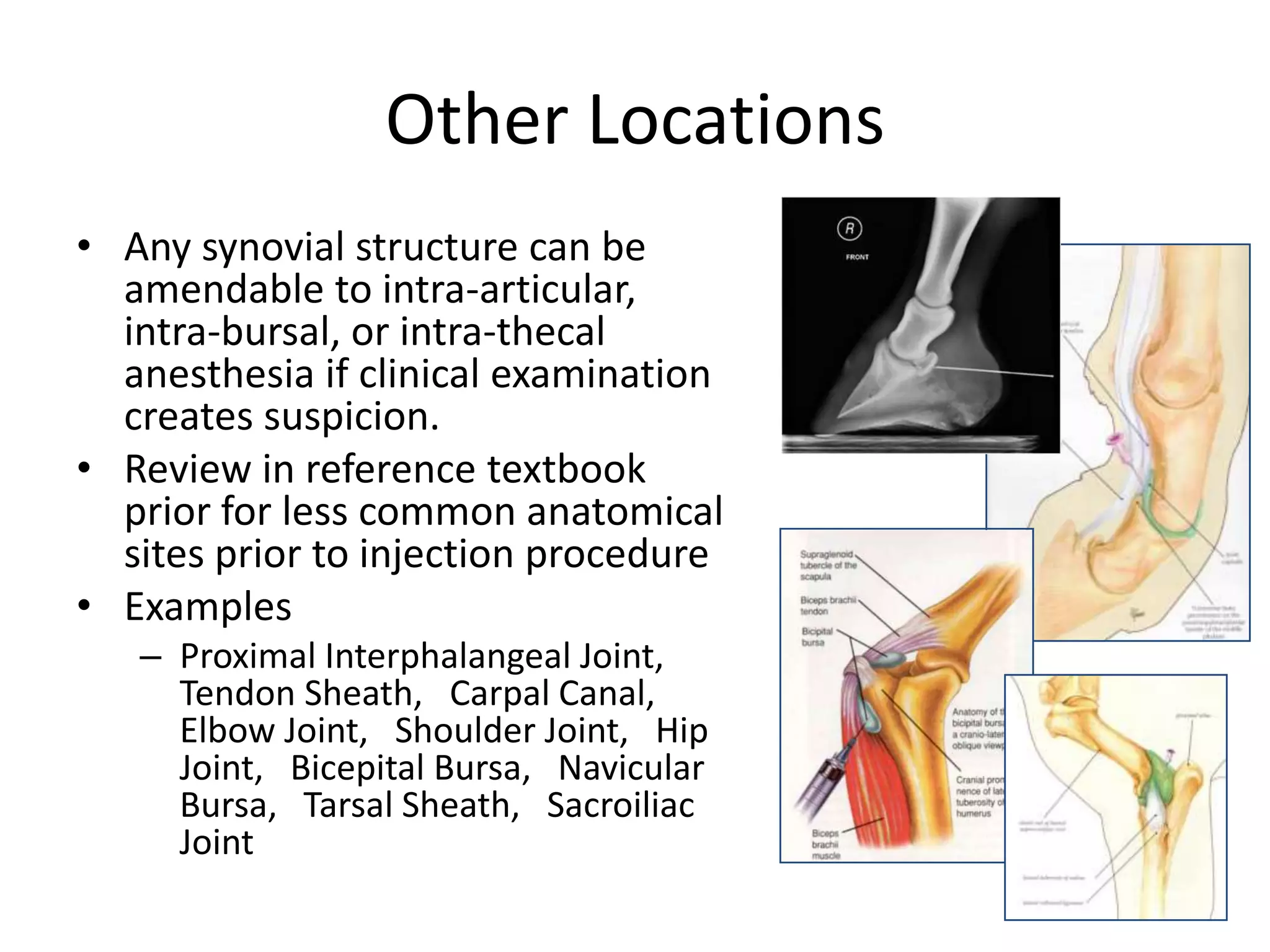


This document discusses nerve and joint blocks in large animals. It provides information on the indications, mechanisms of action, and formulations of local anesthetics used for nerve and joint blocks. Specific techniques are described for performing nerve blocks of various nerves in the limbs, as well as joint blocks of the coffin joint, fetlock joint, carpus, tibial-tarsal joint, and stifle joint. The document emphasizes the importance of anatomical knowledge and reviews considerations for determining if a block is effective and potential complications.























































































