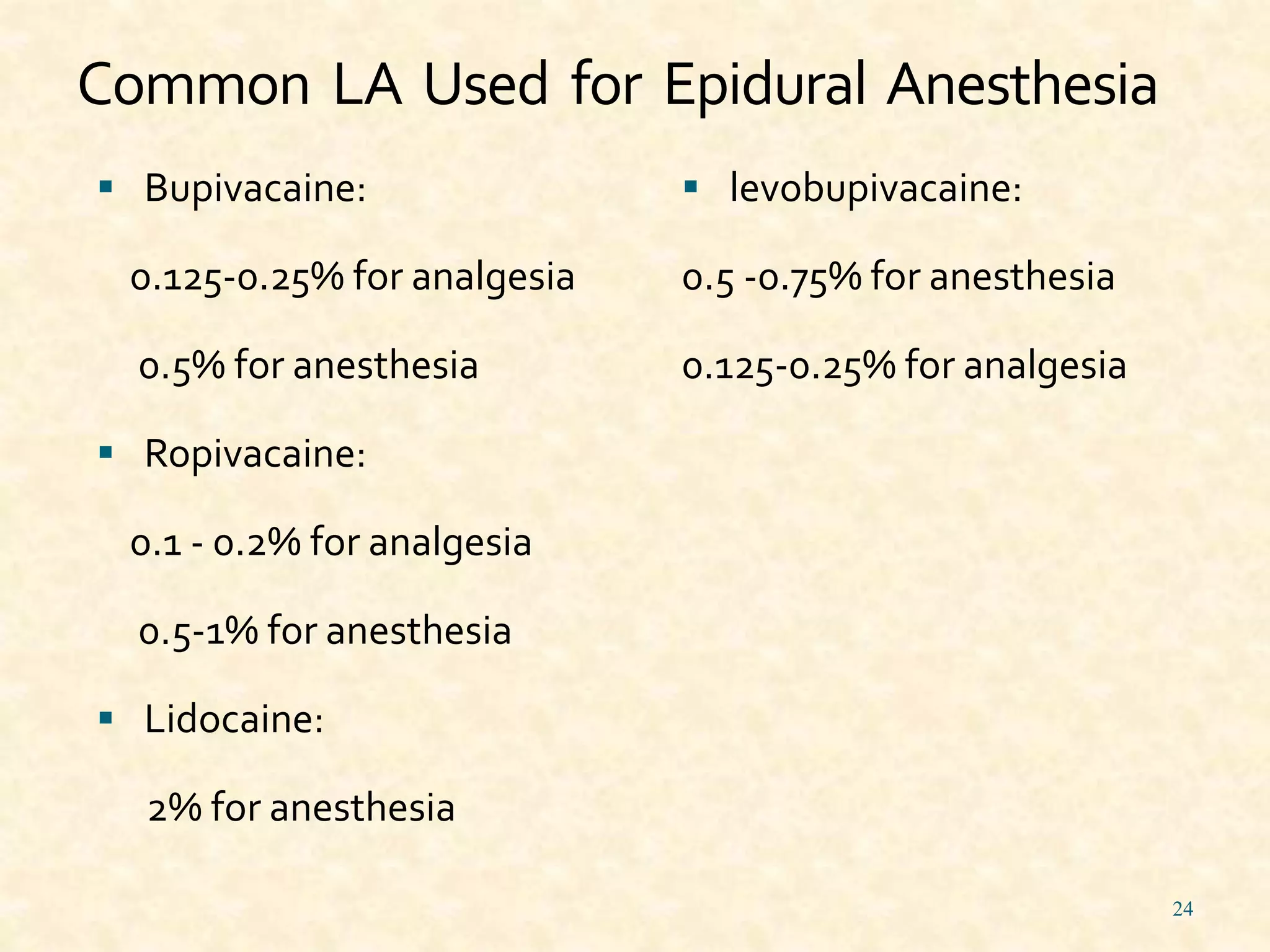
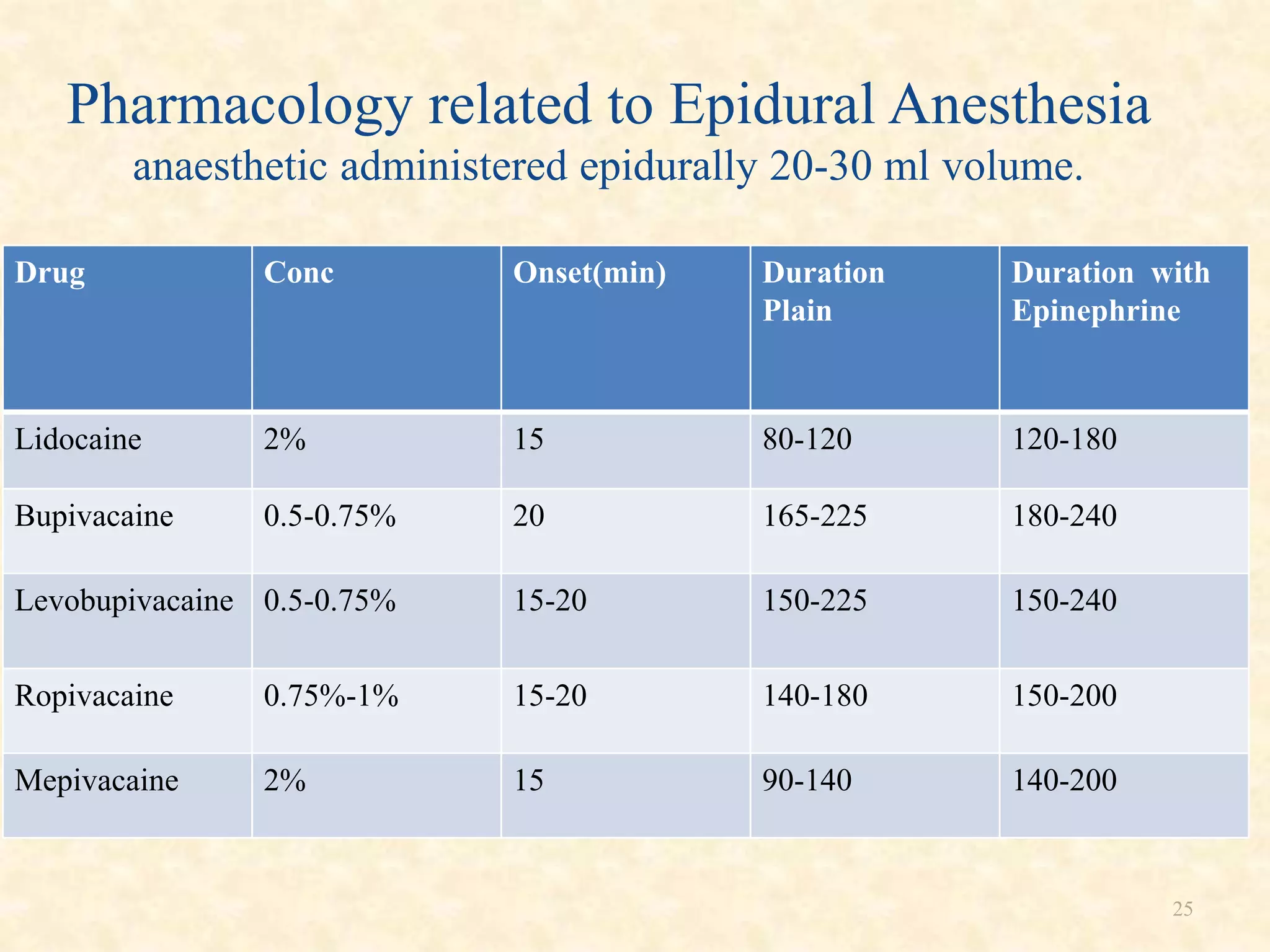
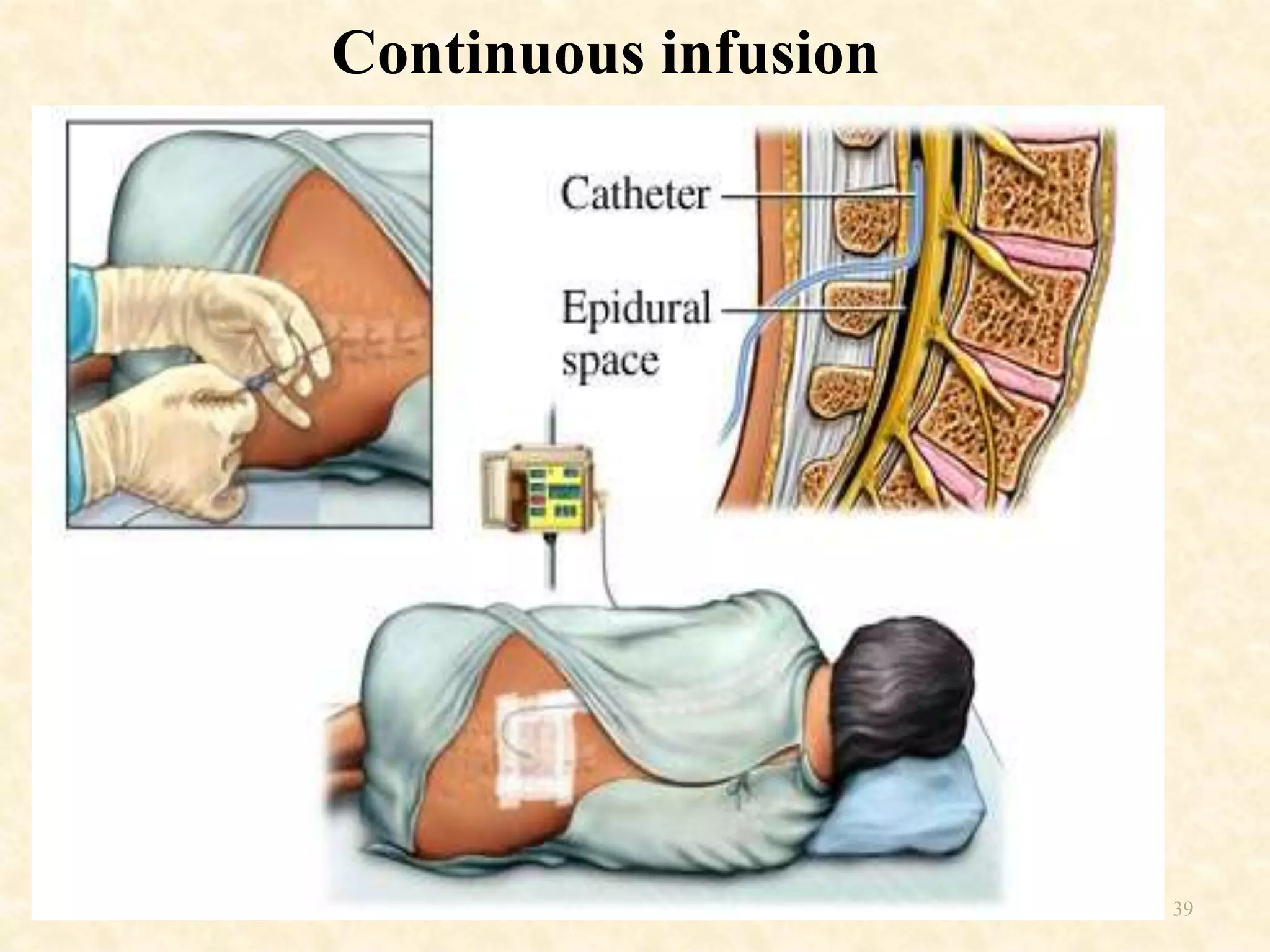
Epidural anesthesia is a neuraxial technique that involves injecting local anesthetic into the epidural space surrounding the dural sac and spinal cord. It provides a wide range of applications including operative anesthesia, obstetric anesthesia and analgesia, postoperative pain control, and chronic pain management. Factors such as the site of injection, dose, age, and weight of the patient can impact the spread and effects of epidural anesthesia. Proper technique and monitoring are required to administer epidural anesthesia safely and effectively.