Download as PDF, PPTX


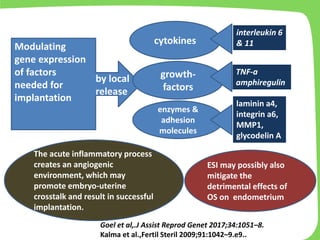
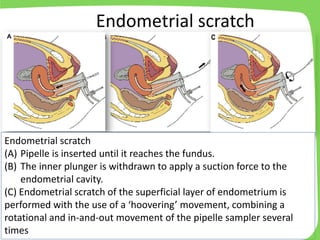




- The document discusses endometrial scratch, a proposed intervention to improve endometrial receptivity and implantation in women undergoing IVF. - Endometrial scratch involves mechanically manipulating the endometrium through procedures like using a pipelle or curette to cause a local injury. This is thought to stimulate an inflammatory response and improve the endometrial environment. - Several studies have found endometrial scratch improved clinical pregnancy and live birth rates, while others found no effect. Meta-analyses show conflicting results due to the low quality of included randomized trials. - The safety, optimal timing and patient population for endometrial scratch require more rigorous research before it can be routinely recommended.



































































