Downloaded 47 times

![…so we can remove impediments
to autonomy and let patients
practice it
“[Once] impediments [to autonomy] are gone, [it is
assumed] people will naturally gather evidence about
the risk and benefits of each medical choice, apply
their values to that evidence, and reach a considered
decision” (Schneider)
Encouraging Patient Autonomy From Theory to
Practice: Z. Berger, Berman Seminar, 2/27/2012
3](https://image.slidesharecdn.com/encouragingpatientautonomy-120305084259-phpapp01/85/Encouraging-patient-autonomy-3-320.jpg)






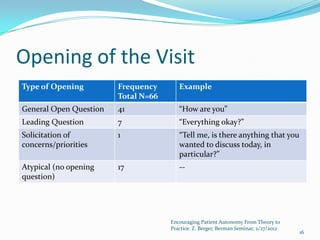
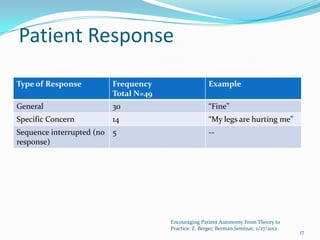
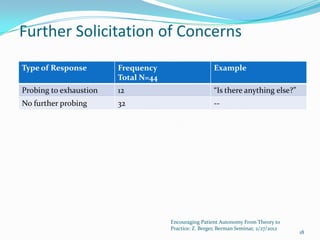











Zackary Berger gave a seminar on encouraging patient autonomy in practice. He discussed how patient autonomy is viewed in theory as patients evaluating treatment options based on their own values, but in reality patients often do not feel able to make autonomous decisions. The study examined how physicians elicit patient concerns in HIV clinic visits. It found that generic opening questions did not effectively elicit concerns, and physicians did not typically probe further after patients responded that they were "fine". When setting visit agendas, physicians often directed the agenda rather than exploring patient priorities.






































![Test taking[1] mw](https://cdn.slidesharecdn.com/ss_thumbnails/testtaking1mw-111216123635-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































