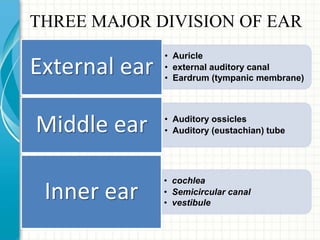
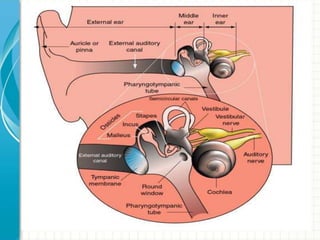
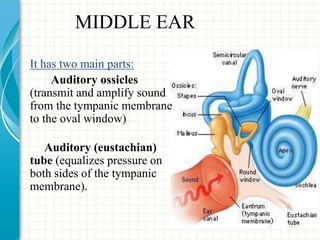
The ear can be divided into three main sections:
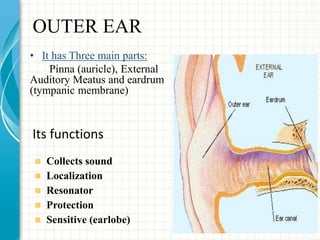
1. The outer ear collects sound waves and directs them to the eardrum.
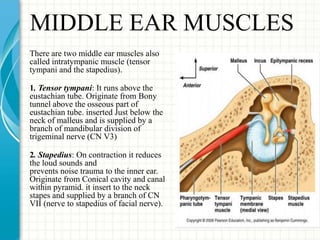
2. The middle ear contains three small bones that amplify vibrations and transmit them to the inner ear. It also contains two muscles and two nerves.
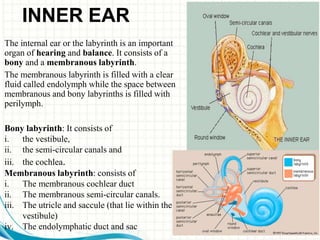
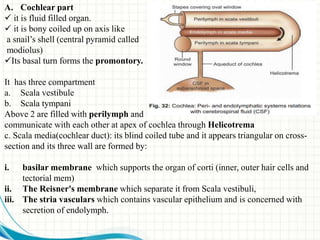
3. The inner ear contains the cochlea for hearing and semicircular canals for balance. Within the cochlea is the organ of Corti which contains hair cells that transduce sound vibrations into nerve signals.