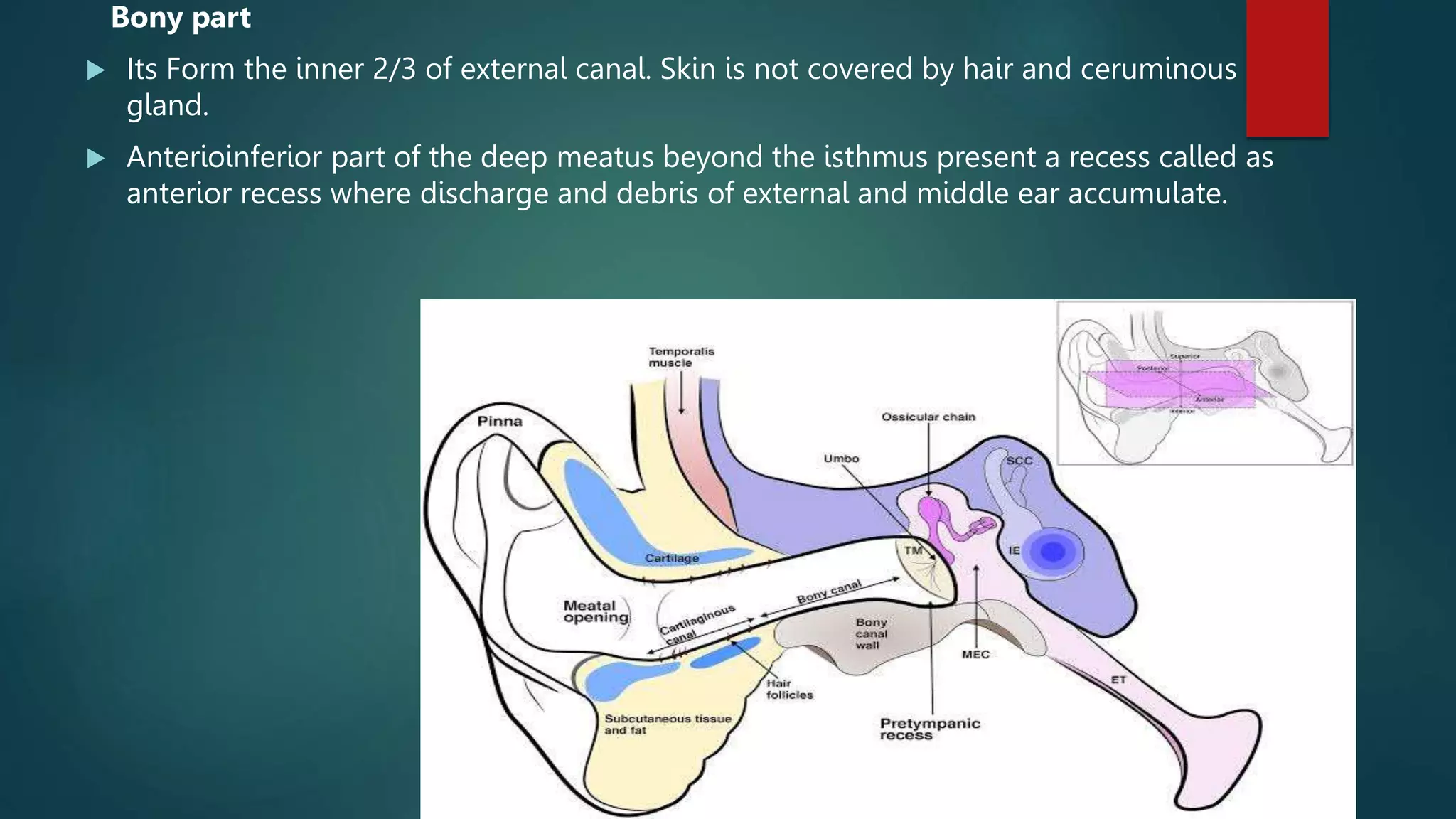
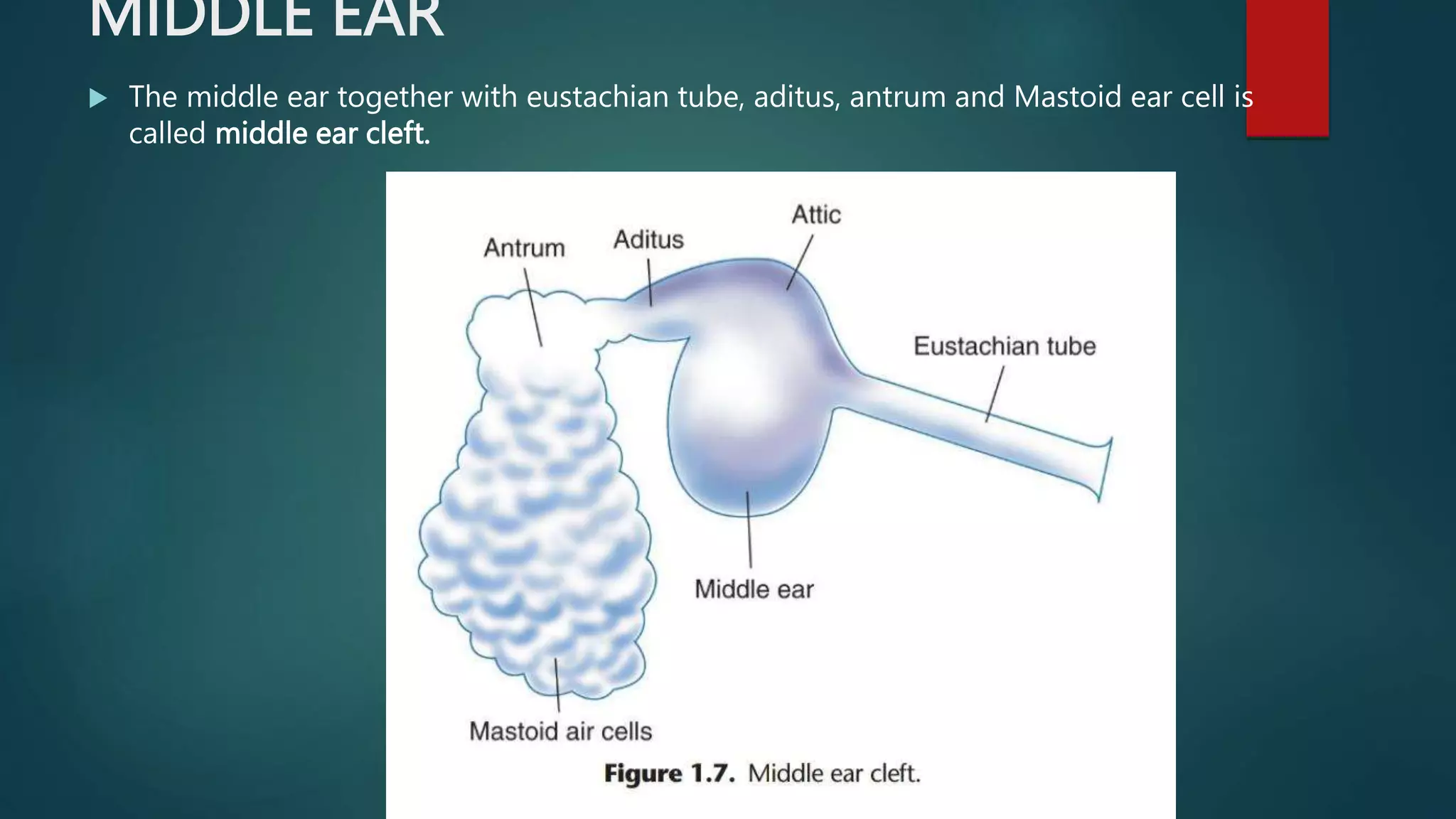
The document summarizes the anatomy and physiology of the ear. It is divided into three main parts: the external ear, middle ear, and inner ear. The external ear collects sound waves and directs them through the external auditory canal to the tympanic membrane. The middle ear contains three small bones (ossicles) that transmit sound vibrations from the tympanic membrane to the inner ear. The inner ear, or labyrinth, contains the cochlea for hearing and semicircular canals for balance. It converts sound vibrations into neural signals that are sent to the brain.

















































![pterygopalatine_fossa_and_its_approachs[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pterygopalatinefossaanditsapproachs1-231217010847-cfbc0b0a-thumbnail.jpg?width=640&height=640&fit=bounds)
































































