Downloaded 241 times
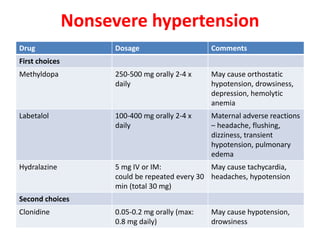
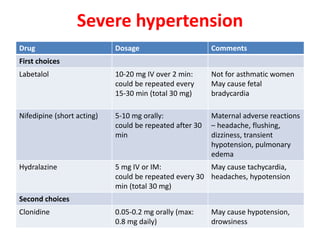
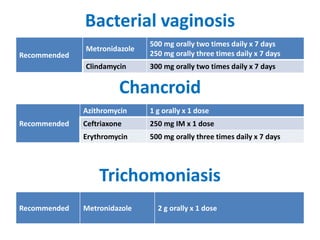
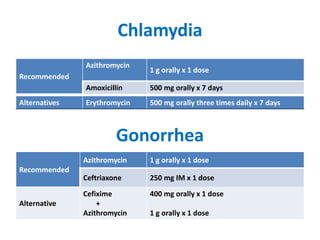
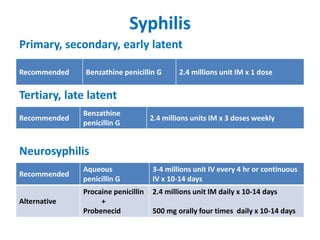
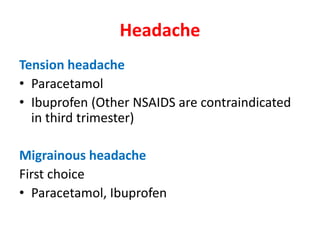


This document discusses drug use and management of common medical conditions during pregnancy. It covers gastrointestinal issues, gestational diabetes, hypertensive disorders, thyroid abnormalities, thromboembolism, urinary tract infections, sexually transmitted infections, headache, malaria, tuberculosis, asthma, allergic rhinitis, diabetes, epilepsy, HIV, preterm labor, and antibiotics used during pregnancy. For each condition, it provides recommendations for first-line and alternative drug treatments as well as contraindicated medications. References for the information are also included.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



