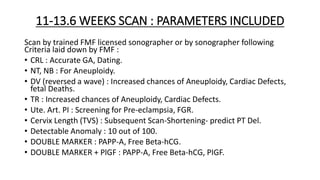
- The document discusses first trimester screening (FTS), which involves an NT scan and serum biochemistry between 11-13.6 weeks of pregnancy.
- FTS allows for early prediction, prevention, diagnosis and management of complications like aneuploidies, preeclampsia, fetal growth restriction, and preterm birth.
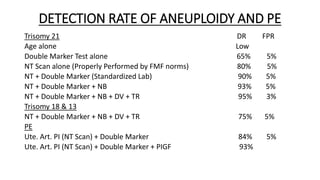
- The NT scan measures nuchal translucency thickness, which is increased in fetuses with chromosomal abnormalities. Combined with blood tests, FTS can assess risk for conditions like Trisomy 21, 18, 13, preeclampsia and more.


![WHAT TO SCREEN FOR? WHY SCREEN?
1] FOR ANEUPLOIDY e.g. Trisomy 21, 18, 13 :
• Many abort , few have IUFD (Stillbirth).
• Trisomy 18, 13 : Survive only for few hours or days after birth.
• Trisomy 21 : may live upto 49 years, but MR, health problems, financial burden.
2] FOR PRE-ECLAMPSIA & FGR :
• PE – Increased Maternal Mortality, Morbidity.
• FGR- Increases IUFD (Stillbirth), MAS, Neonatal Morbidity.
3] FOR PRETERM BIRTH : Increased Neonatal Mortality, Morbidity.
4] SELECTED CONGENITAL ANOMALIES DETECTABLE AT 11-14 WEEKS :
• Only 10 out of 100.
• Counsel : Compatible with life? Surgery required? Prognosis. Decision making.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-5-320.jpg)

![Progressive shortening of length of Cervix or funneling of Cervix or
length < 25 mm on TVS, indicates high risk of Preterm birth/Second
Trimester loss.
So what can be done for that?
1] Cervical Cerclage (Tightening of Os) Operation.
OR
2] Progesterone ( 400 mg vaginally daily at bedtime) till 34 or 36 weeks
of pregnancy.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-13-320.jpg)
![POST TEST COUNSELING FOR PRE-ECLAMPSIA & FGR
Low risk – reassure – Routine Antenatal Care.
High risk – Offer Tab. Aspirin 150 mg/day till 34-36 weeks.
POST TEST COUNSELING FOR PRETERM BIRTH
If previous history of Preterm Birth or HSO Insufficient Cervix or Cervix
Length < 25 mm on TVS or Shortening noticed in subsequent scans :
OFFER
1] Cervical Cerclage : Tightening of OS operation. Or
2] Progesterone 400 mg/day vaginally till 36 weeks.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-20-320.jpg)
![FAQs AFTER FTS : 11-13.6 WEEKS SCREENING
1] NT > 3 mm – Increased chromosomal & structural abnormality – why
not do MTP directly?
• In certain % of cases, NT may resolve after 14 weeks – Normal
Outcome. NT scan is a screening test.
• Diagnostic Test (CVS or Amniocentesis) is important for KT, important
to help parents in decision making & also define recurrence risk.
2] NT > 3 mm & major structural anomaly, why not do MTP directly?
• Diagnostic Test – find out Etiology of Increased NT & calculate
recurrence risk of that condition.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-26-320.jpg)
![3] FTS is low risk, so is everything fine?
• Congratulations. FTS has shown low risk, which is quite reassuring.
Very very small % of false negative may be there.
Friends, as far as structural anomalies are concerned at this stage, CRL
is only 6 cm & only 10 out of 100 anomalies can be detected at this
stage, so Anomaly Scan at 18-22 weeks is the next step. Some evolving
anomalies can be detected in 3rd trimester/after birth.
4] What will be the Recurrence Risk of Aneuploidy/Structural Anomaly?
• Depends on the Aneuploidy or Structural Anomaly Diagnosed.
5] What is the role of Quadruple Marker Test in Screening?
• It might have some role in those who missed FTS for some reason.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-27-320.jpg)
![FUTURE OF FTS
1] Will NIPS replace NT Scan (11-13.6 weeks scan)?
• No, NIPS can only predict Aneuploidy risk, NT Scan can do 4 more
things.
2] Will NIPS replace Dual Marker Test?
• Yes it will, as it has higher DR (Sensitivity), When? As soon as the cost
comes down.
3] FUTURE WILL BE ‘SUPPEMENTARY FTS or TESTING’ ie. NT Scan +
NIPS.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-28-320.jpg)
![Remember 3 things :
1] For FTS, proper Pre Test & Post Test Counseling & following a
protocol are very important.
2] FTS today is NT + Double Marker Test.
3] FTS tomorrow will be NT + NIPS.](https://image.slidesharecdn.com/ntscans-221211070001-3739040c/85/NT-SCAN-11-13-6-weeks-Serum-BIOPROFILE-29-320.jpg)