Downloaded 134 times


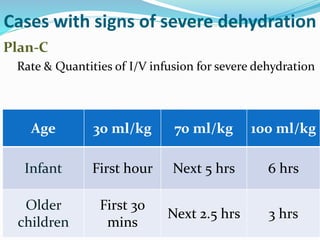





This document provides an overview of diarrheal disease including its causes, classification, management, and prevention. It discusses that diarrheal disease is the second leading cause of death in children under 5 globally. The main points are: acute watery diarrhea accounts for over 75% of cases; continued feeding and oral rehydration solutions are the primary treatment; zinc and probiotics can help prevent and treat diarrhea; and diarrhea management should focus on preventing dehydration through oral rehydration.






















































































