Downloaded 61 times


![• DIABETES TECHNOLOGY INCLUDES THE HARDWARE, DEVICES, AND SOFTWARE
THAT PEOPLE WITH DIABETES USE TO HELP MANAGE THEIR DIABETES.
THIS INCLUDES INSULIN DELIVERY TECHNOLOGY SUCH AS INSULIN PUMPS (ALSO
CALLED CONTINUOUS SUBCUTANEOUS INSULIN INFUSION [CSII]) AND
CONNECTED INSULIN PENS, AS WELL AS GLUCOSE MONITORING VIA CGM
SYSTEM OR GLUCOSE METER.
MORE RECENTLY, DIABETES TECHNOLOGY HAS EXPANDED TO INCLUDE HYBRID
DEVICES THAT BOTH MONITOR GLUCOSE AND DELIVER INSULIN, SOME WITH
VARYING DEGREES OF AUTOMATION. APPS CAN ALSO PROVIDE DIABETES SELF-
MANAGEMENT SUPPORT](https://image.slidesharecdn.com/diabetestechnology-220315083354/85/Diabetes-technology-2-320.jpg)
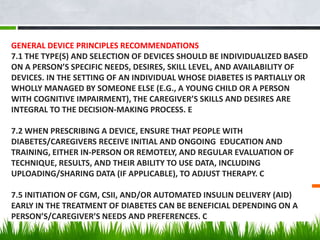

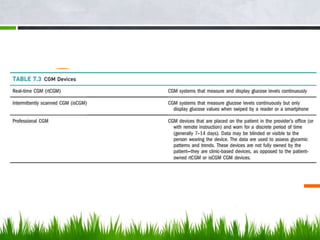



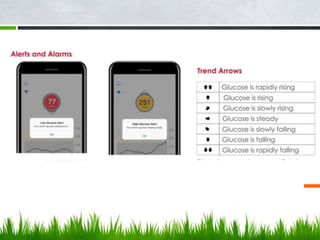


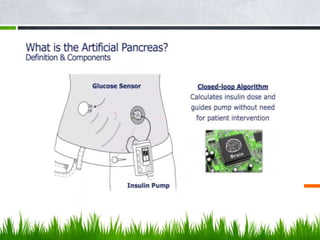





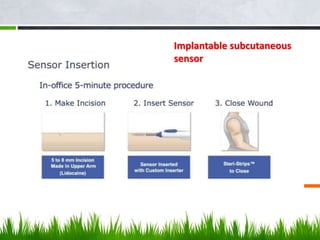

This document discusses diabetes technology including continuous glucose monitoring (CGM) systems, insulin pumps, and smart pens. CGM systems can monitor glucose levels in real-time or intermittently and have been shown to help lower A1C levels and reduce hypoglycemic episodes when used regularly. Insulin pumps can also help improve glucose control and reduce complications compared to multiple daily injections. While this technology has benefits, it also has costs and limitations, so expectations must be managed. Future diabetes devices may include implantable sensors, combined insulin and glucagon delivery, but self-care will still be required to manage the disease.































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





