
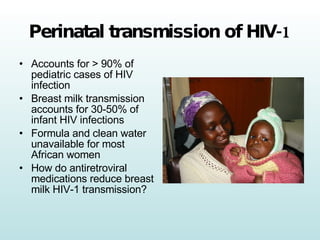










The document discusses the implementation of HIV research and clinical trials in Kenya, particularly focusing on perinatal HIV-1 transmission and the effectiveness of various antiretroviral therapies. It highlights the significant gap in treatment access for HIV-infected individuals in Kenya, the role of academic medicine in addressing global health needs, and the importance of local interventions. The findings underscore that field-based research and practice can lead to improved treatment strategies and health outcomes for affected populations.























































































