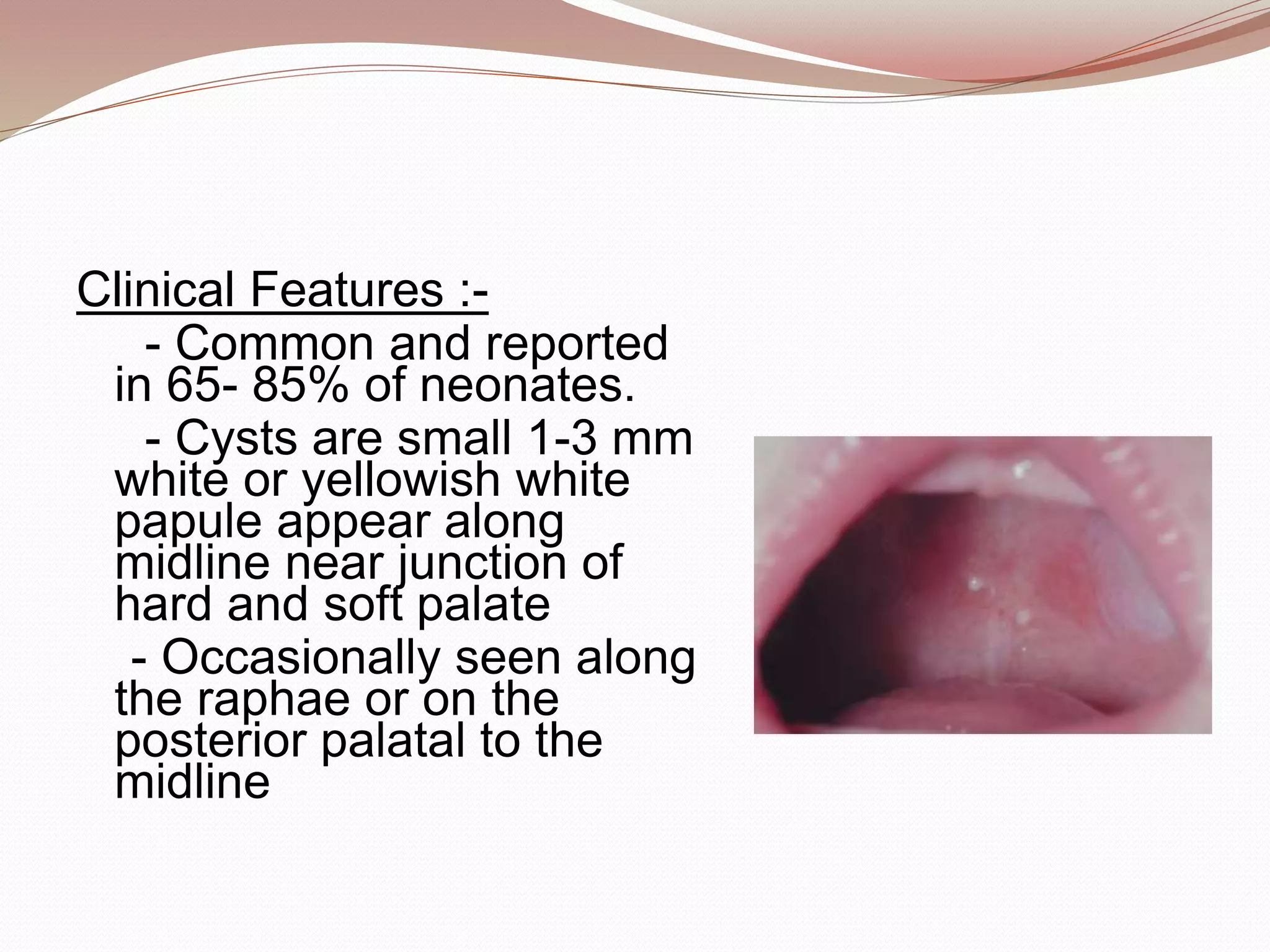
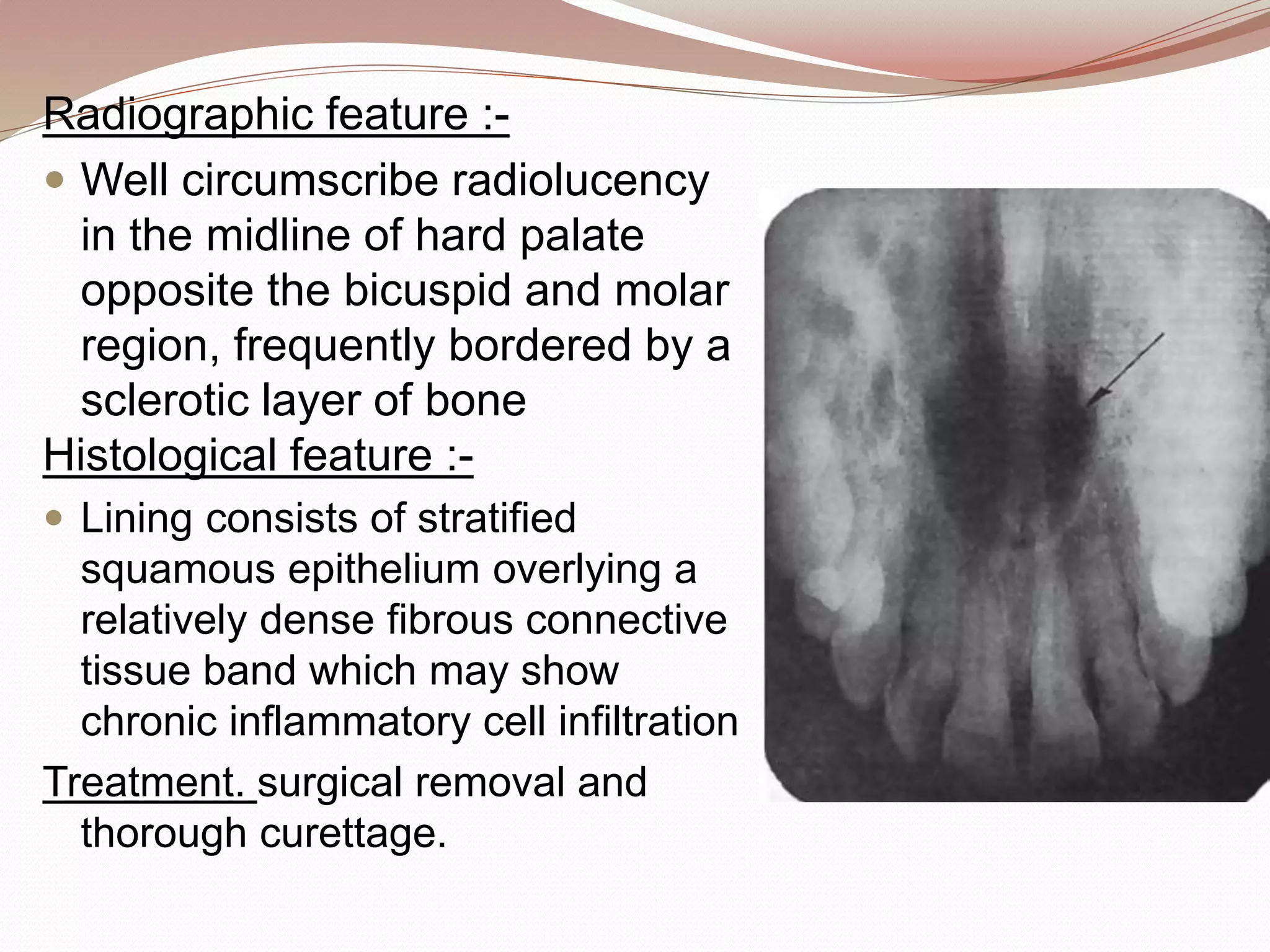
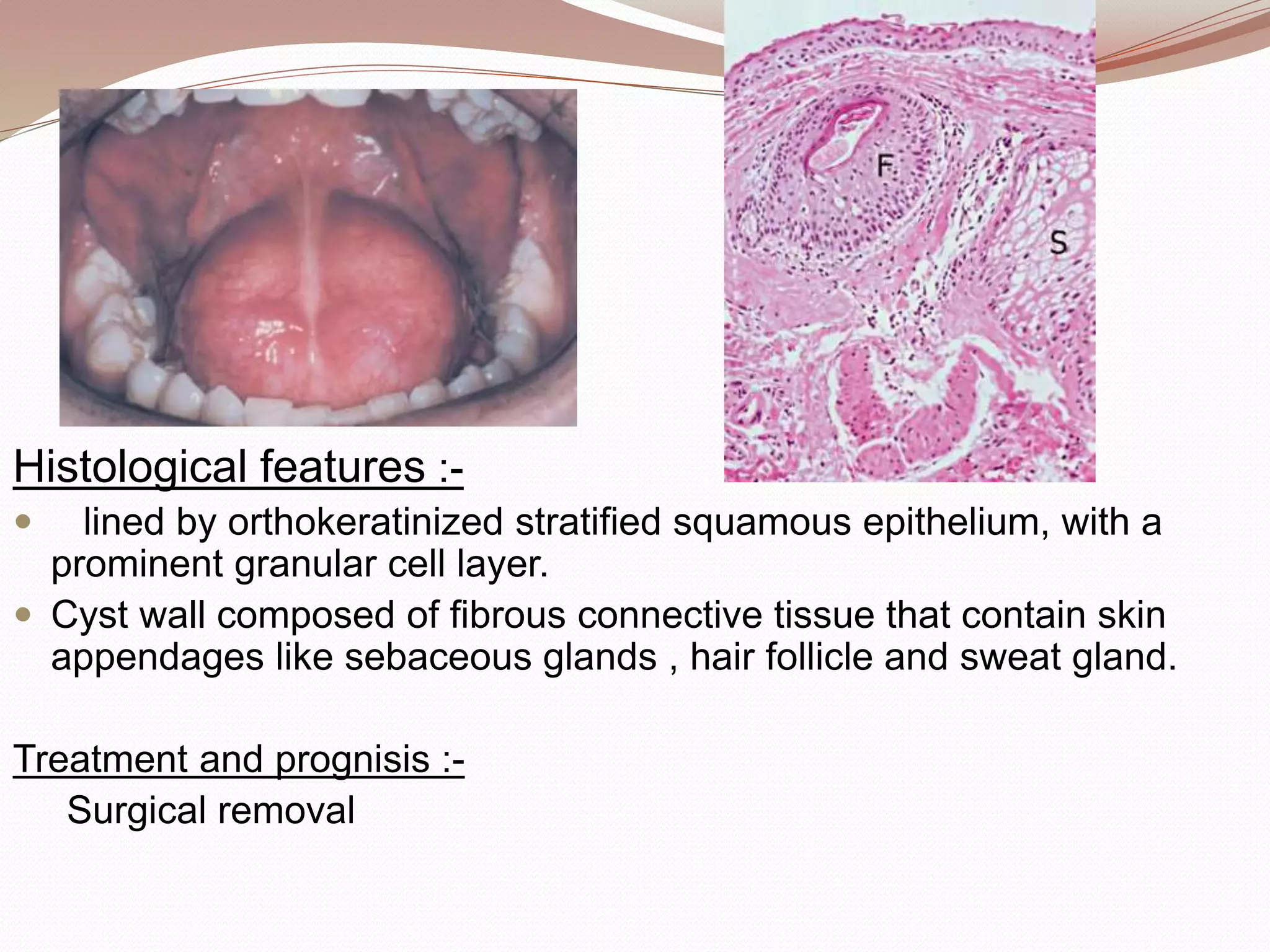
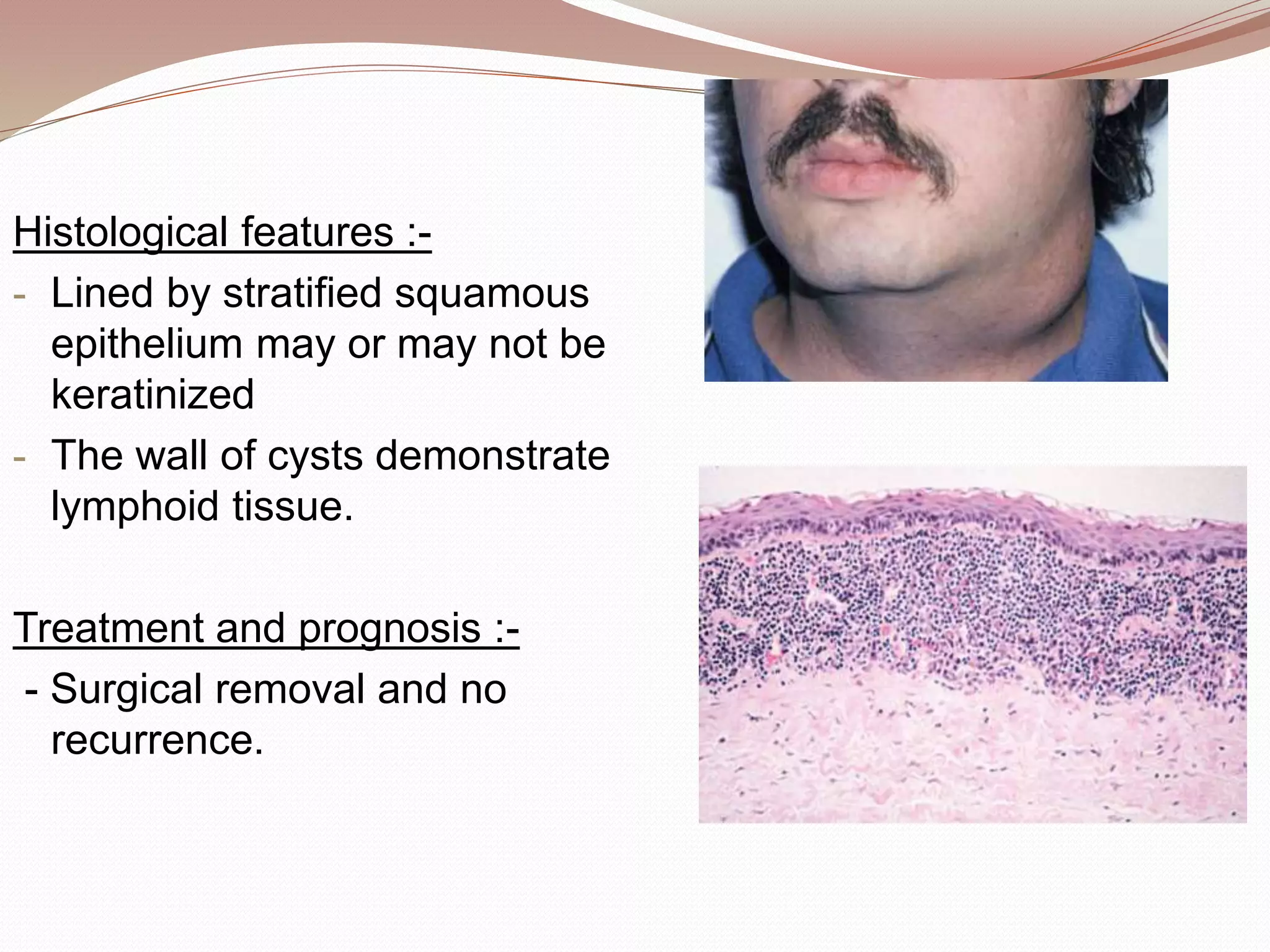
This document discusses various developmental cysts that can occur in the oral and maxillofacial region. It provides details on the location, cause, clinical features, radiographic features, histological features, treatment and prognosis for different cysts such as palatal cyst of newborn, nasolabial cyst, globullomaxillary cyst, nasopalatine duct cyst, median palatal cyst, median mandibular cyst, epidermoid cyst, dermoid cyst, thyroglossal duct cyst, branchial cleft cyst, and oral lymphoepithelial cyst.