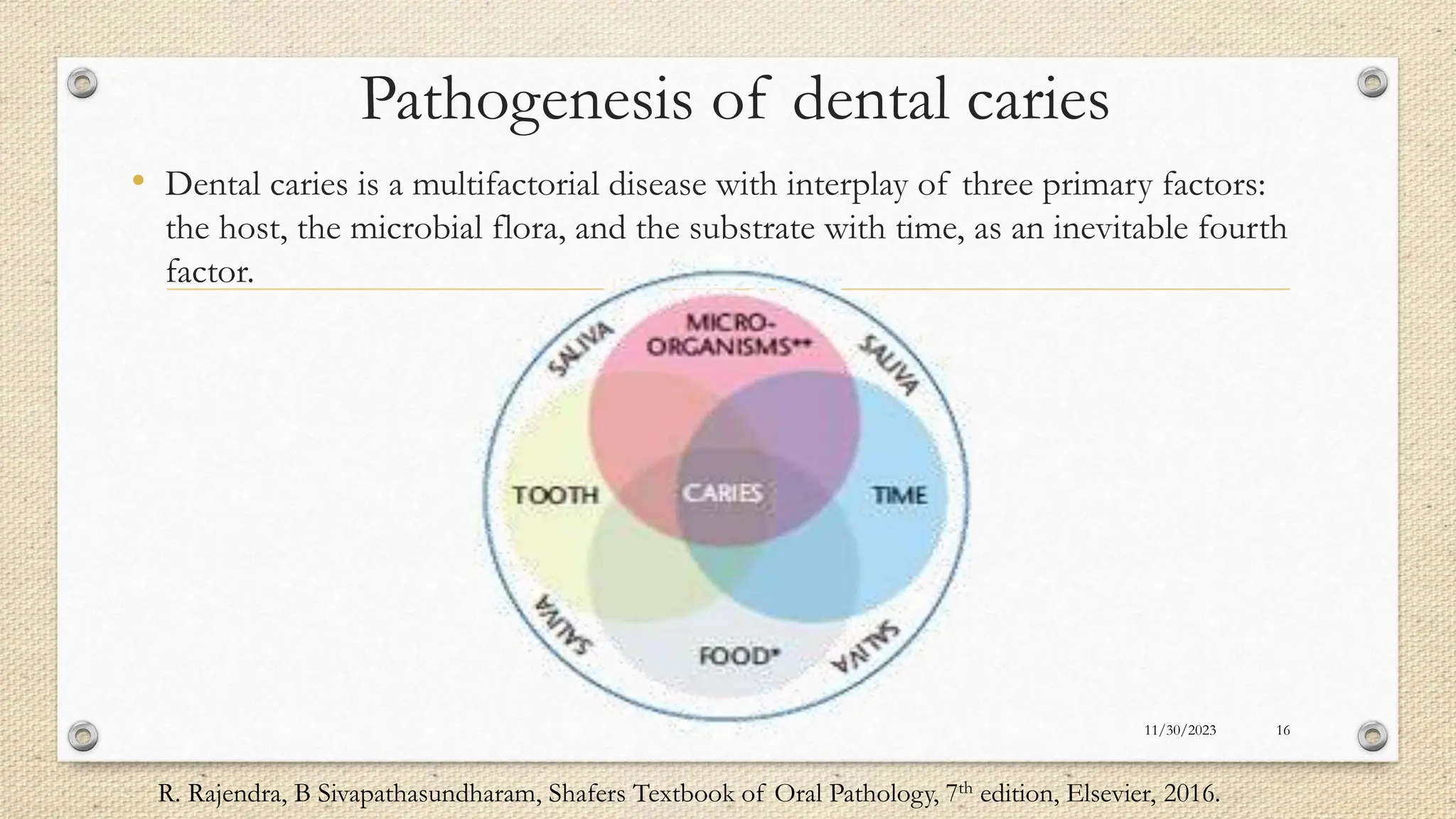
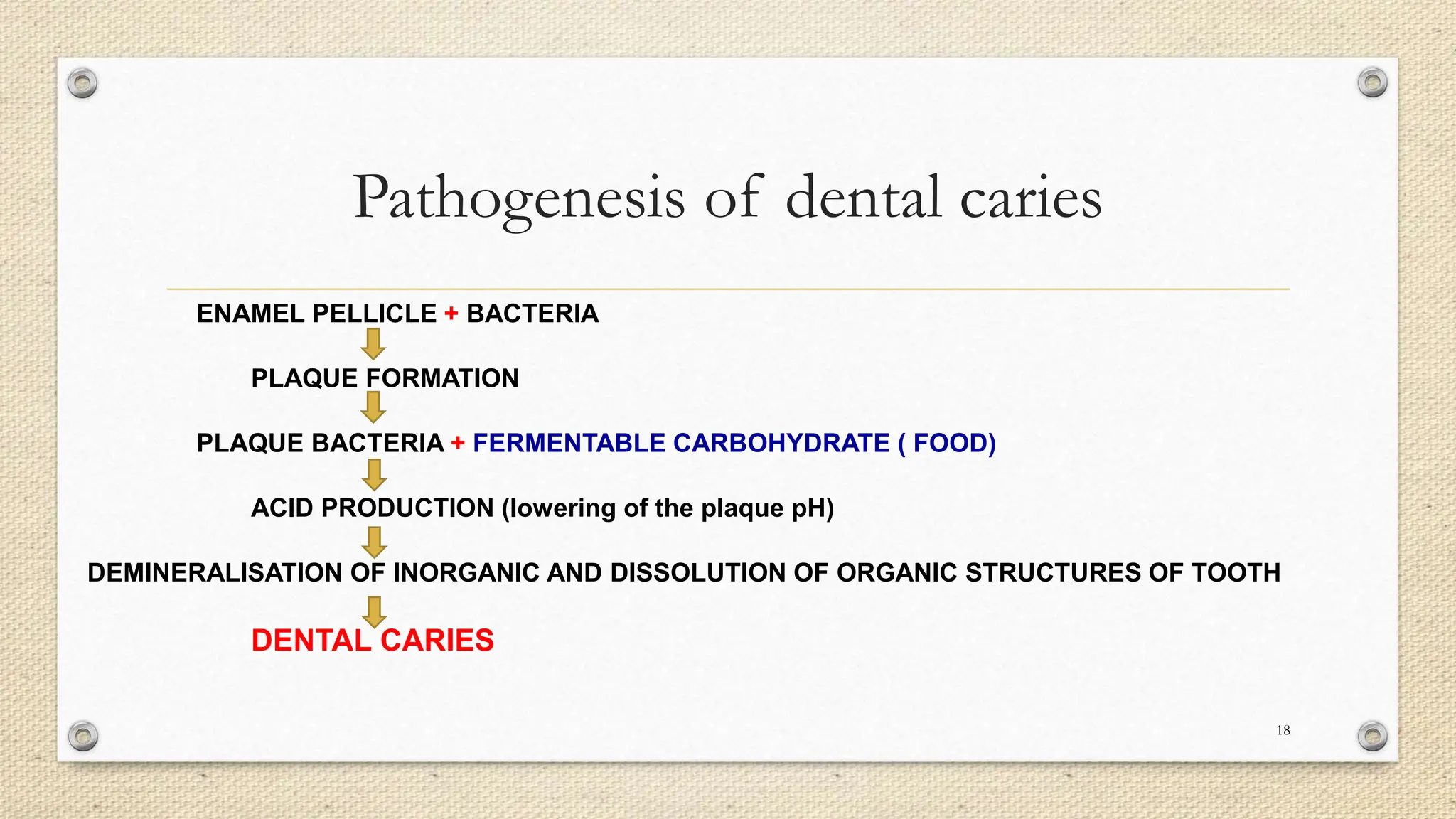
The document discusses the relationship between diet and dental caries, defining dental caries as an infectious microbial disease leading to tooth decay. It illustrates the multifactorial aetiology of caries, emphasizing the impact of dietary habits, particularly the consumption of fermentable carbohydrates, on tooth health. Additionally, it presents various theories and studies linking dietary patterns to the prevalence of dental caries, highlighting the importance of preventive measures and dietary counseling.