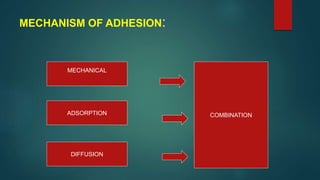
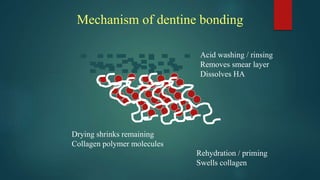
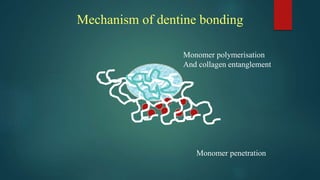
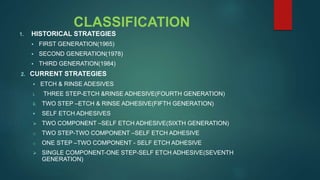
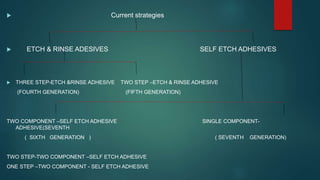
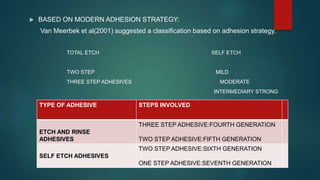
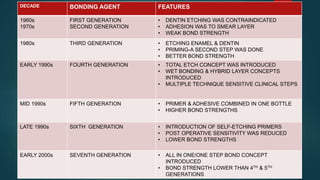
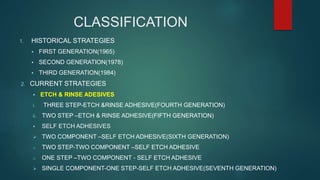
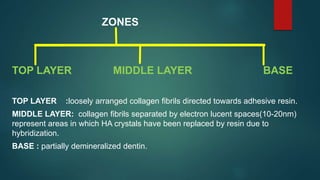
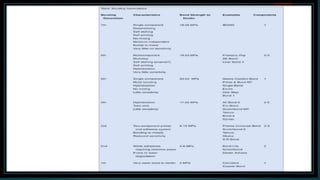
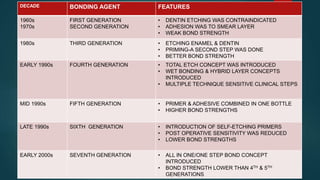
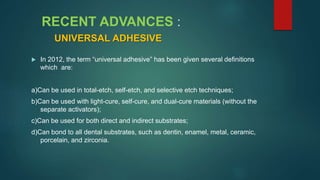
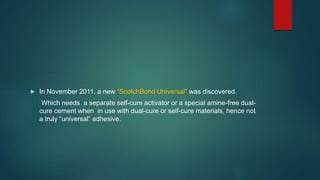
The document discusses the role and importance of adhesive dentistry. It describes the different generations of dentine bonding agents from the early phosphoric acid-based systems to newer self-etch adhesives. Key challenges in dentine adhesion are the structural differences between enamel and dentine such as dentine's high water content and presence of a smear layer. Conditioning with acid or chelators is needed to remove the smear layer and expose collagen fibers for bonding to occur. Current adhesive systems are classified as etch-and-rinse or self-etch and involve either two or three step application processes.



























![Dental Casting alloys [DENTAL MATERIALS]](https://cdn.slidesharecdn.com/ss_thumbnails/castingalloysbp-200331155134-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































