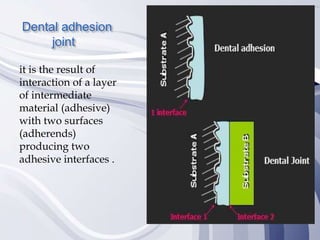
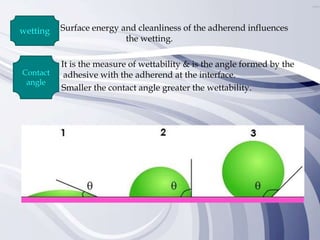
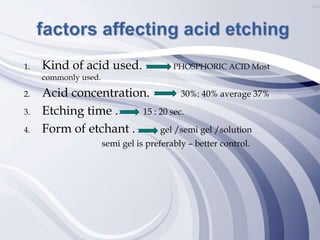
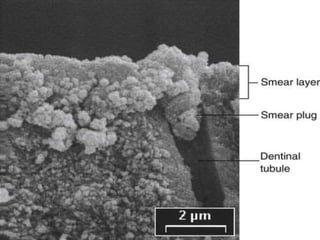
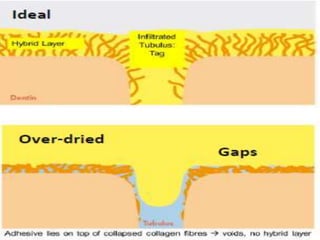
Adhesion in dentistry involves bonding dental materials such as composites to tooth structure. There are two main types of adhesion - chemical and micromechanical. Chemical adhesion involves bonding between tooth and material molecules while micromechanical adhesion uses surface irregularities created by etching to mechanically interlock the material. Factors like surface energy and cleanliness influence adhesion. Conditioning times for enamel and dentin can affect bond strength, with some studies finding extended times increase strength for dentin but not enamel. High quality adhesion improves restoration retention and resistance to leakage and fracture.