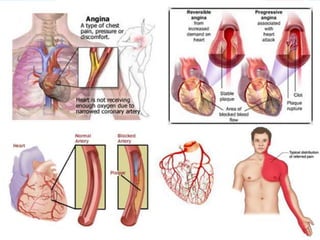
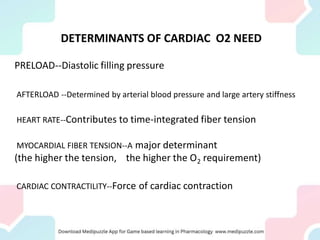
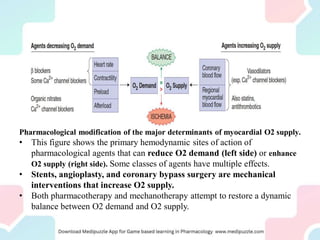
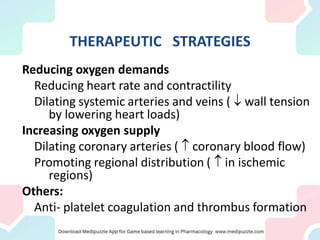
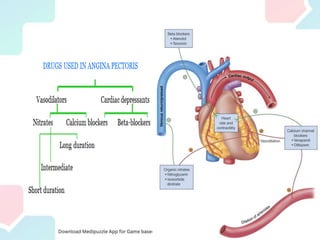
Angina pectoris, a key symptom of ischemic heart disease, results from an imbalance in myocardial oxygen supply and demand, leading to chest pain. It can be classified into exertional, variant, and unstable angina, with various therapeutic strategies employing pharmacological agents, mechanical interventions, and lifestyle changes to restore balance. Treatment options include nitrates, beta-blockers, and calcium channel blockers, each acting to reduce oxygen demand or enhance supply, with attention to potential side effects and contraindications.































![Anti-angina_F.K.ppt_for_midwife[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anti-anginaf-230902073731-f0ce562d-thumbnail.jpg?width=640&height=640&fit=bounds)


























































