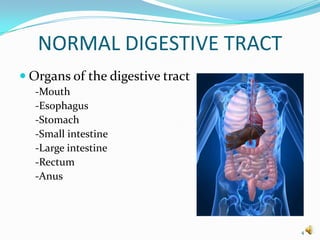
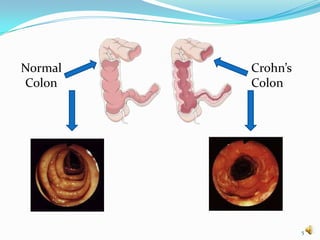
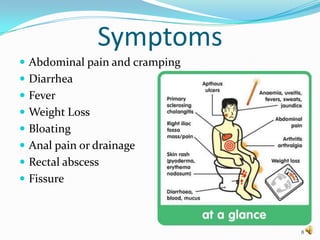
This document provides information about Crohn's disease, including what it is, symptoms, causes, risk factors, diagnosis, treatment, and living with the disease. Specifically, it defines Crohn's as a chronic inflammatory disease of the gastrointestinal tract that causes ulceration of the intestines. It affects the small and large intestines but can occur anywhere in the GI tract. While the exact cause is unknown, theories include issues with the immune system or environmental factors. Treatment involves medications to reduce inflammation and manage symptoms, as well as potential surgery. The document emphasizes that Crohn's is a lifelong condition but one that can be managed with medical treatment and lifestyle changes.