Download to read offline
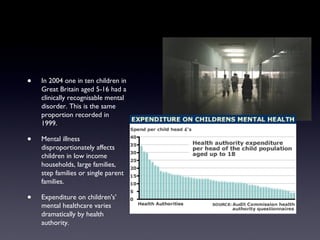
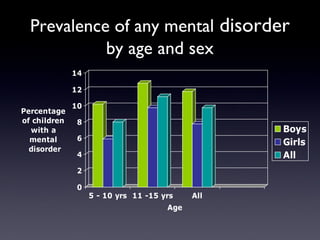
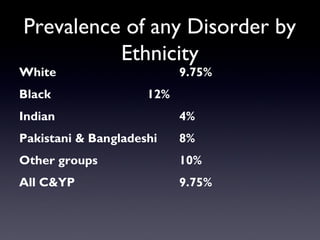
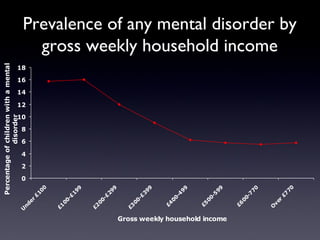

The document provides information on children's mental health, including: - 1 in 10 children in the UK have a clinically diagnosed mental disorder, which has remained steady since 1999. Mental illness disproportionately affects children from low-income families or those in non-traditional family structures. - Definitions of mental health focus on the ability to develop relationships, cope with stress, and live a productive life. Young people see family/friends, ability to talk to others, personal achievement, and self-esteem as important for mental wellbeing. - Around 20% of children experience a mental health problem, while 10% have a diagnosable disorder. Rates are higher in older children, some ethnic groups


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)