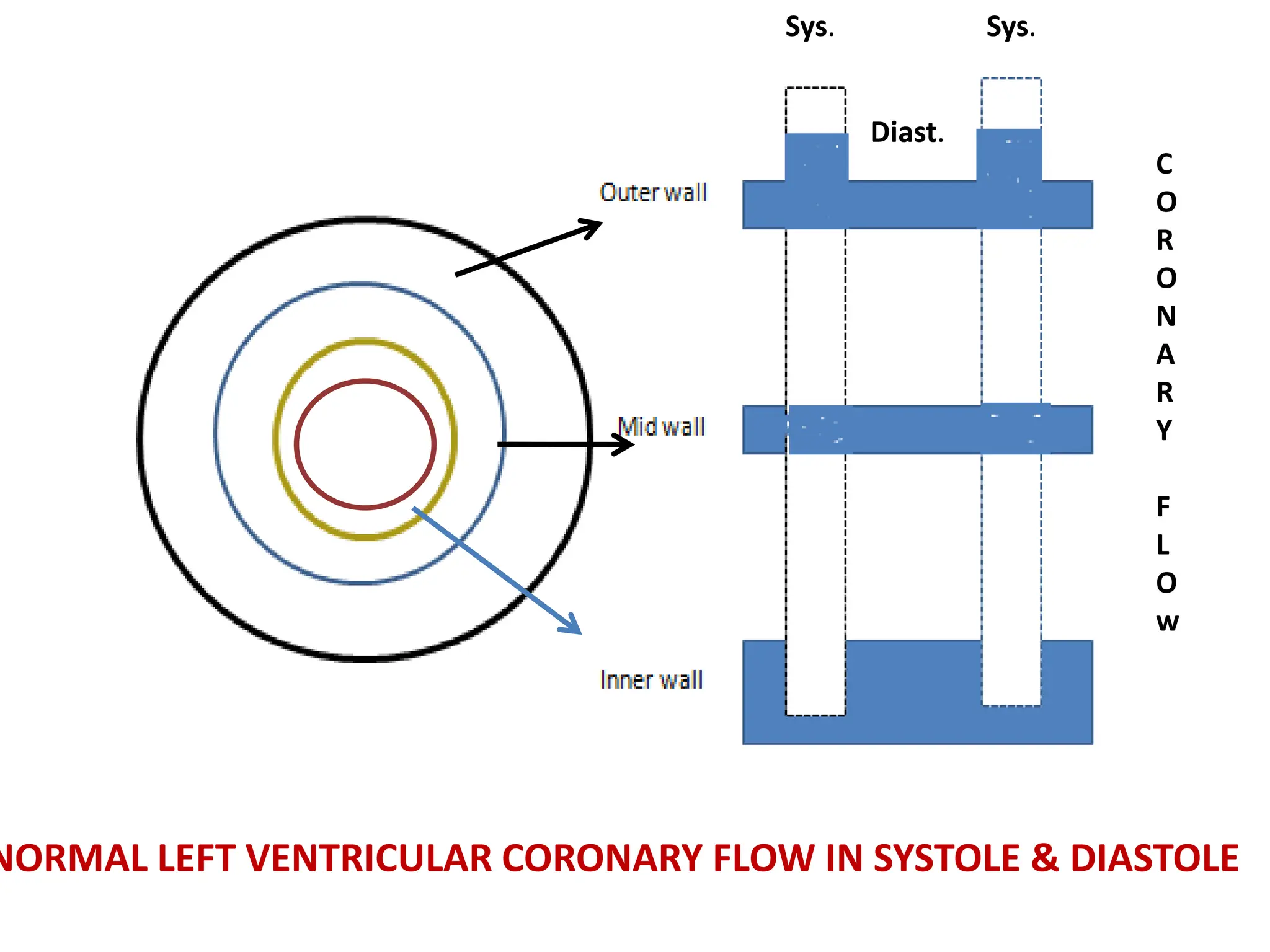
1) Normal coronary blood flow is 60-80 ml/100 gm/min, with 80% occurring during diastole and 20% during systole to accommodate the heart's demand for blood when it is relaxed between contractions.
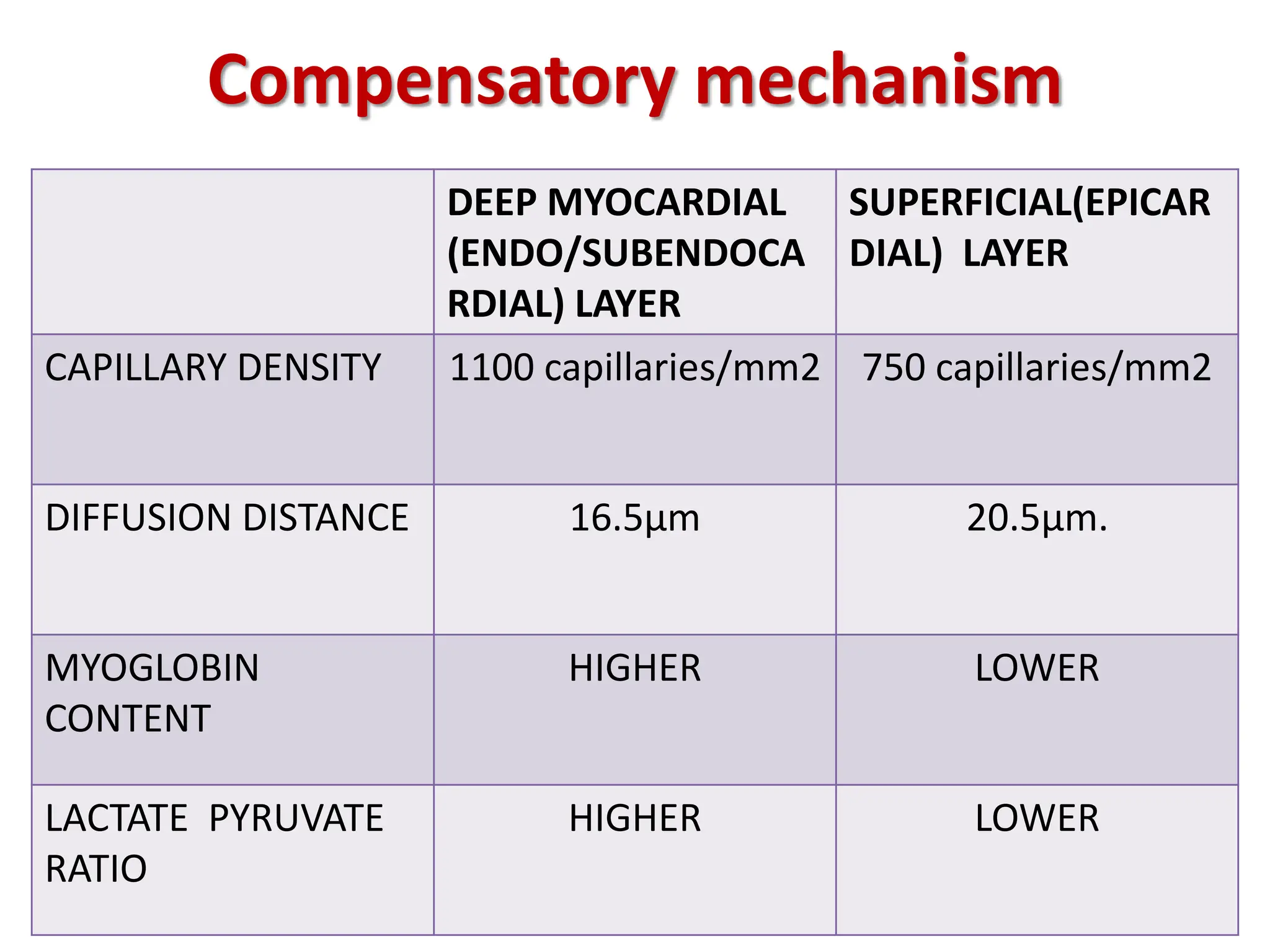
2) The heart has compensatory mechanisms for obtaining oxygen, including deeper capillary layers and higher myoglobin content in the deeper layers to facilitate diffusion during limited flow.
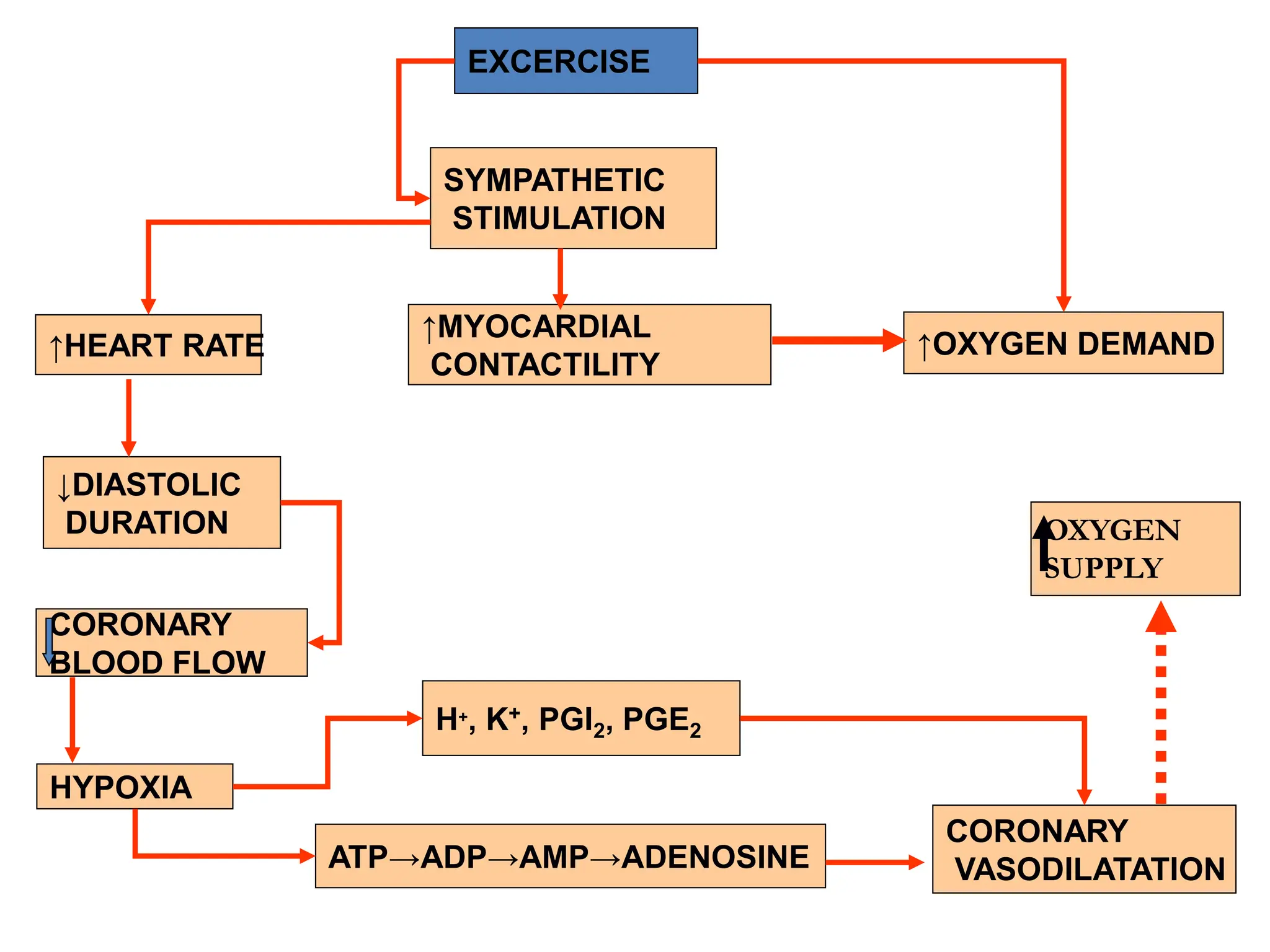
3) Coronary blood flow is regulated both locally, through mechanisms like autoregulation and metabolic factors, and neurogenically through the sympathetic and parasympathetic nervous systems. Increased demand is met by increased blood flow rather than solely by extracting more oxygen.



































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














