EPIDEMIOLOGY
• 4th
leading causeof death (Globally)
• 8th
leading cause of poor health (disability adjusted life years) -
Globally
• 5% of all global deaths in 2021 – 90% of COPD deaths below 70 yrs in
LMIC
• High income countries: 70% cases of COPD – secondary to tobacco
smoking
• LMIC:30-40% COPD cases secondary to smoking. In the remaining -
Household air pollution is a major risk factor
3.
EPIDEMIOLOGY
PAKISTAN
• Current datasuggests: Prevalence in > 40 yrs: 9-10 %
• BOLD epidemiologic study in 2010: 11.7%
• Meta analysis 2018: Pak has highest prevalence in EMRO region
• Increasing prevalence due to increasing smoking trends
4.
INTRODUCTION
COPD is acommon, preventable and treatable disease that is
characterized by persistent respiratory symptoms and airflow limitation
that is due to airway and/or alveolar abnormalities usually caused by
significant exposure to noxious particles or gases and influenced by
host factors including abnormal lung development.
5.
RISK FACTORS
1. Smoking
2.Indoor and outdoor air pollution
3. Genetic predisposition
4. Infections
5. Socioeconomic status
6. Age
7. Gender
6.
SMOKING- PASSIVE
Contribution ofexposure to passive smoking
Prenatal exposure
• o Reduced lung development
• o Low birth weight
Childhood
• o Decreased lung growth
• Adulthood
• o Accelerated decline in lung function
• o Lung destruction
• o Impaired lung repair
7.
SMOKING
• Smokers sufferan irreversible loss of 4.4-10.4 ml in FEV1 per pack year smoked
• Greater the total no of cigarettes – greater the risk of COPD development
• PACK YEARS
• Pack year = Number of cigarettes smoked per day x Number of years of
smoking/20
• Loose tobacco is quantified as tobacco smoked in “ounces per week”, which
can be converted Into pack years
• Pack years = Ounces of loose tobacco per week × 2/7 × number of years
smoked
8.
SMOKING
FUN FACT
• 25-45%of COPD patients are life long non smokers.
• Less than 50% of heavy smokers DO NOT develop COPD
9.
PATHOGENESIS
• In healthyindividuals, the lung shows an inflammatory response to
noxious/irritant particles.
• In COPD this response is modified and pathological changes occur in
airways, the lung parenchyma and the pulmonary vasculature.
• Oxidative stress secondary to smoke
• Protease-Antiprotease imbalance: Inactivation of anti-proteinases
leading to destruction of connective tissue
• Predominance of anti inflammatory cells: macrophages, activated
neutrophils and lymphocytes, eosinophils in mixed COPD/Asthma pts
10.
PATHOGENESIS
• CHRONIC BRONCHITIS
•Chronic cough and sputum for at least 3 months a year for 2
consecutive years.
• (it is now known that chronic bronchitis is a distinct entity that can
exist with or without airflow limitation)
• EMPHYSEMA
• Abnormal permanent enlargement of airspaces distal to the terminal
bronchioles accompanied by destruction of their walls
SYMPTOMS
• Dyspnea
• Coughand sputum
• Wheezing and chest tightness
• Atypical chest pain
• Fatigue
• Psychiatric morbidity esp depression
• Poor sleep quality
• Wt loss ( hall mark of severe disease, poor prognosis)
14.
SYMPTOMS
DYSPNEA
• The hallmarkof COPD is chronic progressive dyspnea.
• Major cause of disability and anxiety associated with the disease. The
breathlessness increases with exertion, and it is there all the time.
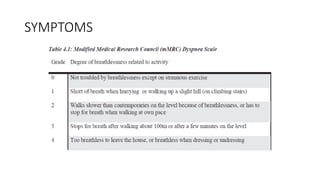
• It can be assessed by using modified Medical Research Council
(mMRC) Dyspnea Scale
SYMPTOMS
COUGH AND SPUTUM
•Can be non productive. Worse in the morning. Small in amount and
whitish in color
• Copious amount of sputum: Underlying Broncheictasis possible
• Persistent purulent sputum: bacterial colonization of airways
(Pseudomonas common)
• Cough syncope, cough fractures of ribs may also occur
17.
SIGNS
• Uniformly diminishedbreath sounds
• Prolonged expiratory phase of breathing
• Purse-lipped breathing
• Use of accessory muscles of breathing
• Barrel-shaped chest
• Horizontal ribs with prominent sterna angle and wide sub-costal angle
• Inspiratory tracheal tug
• Hoover’s sign – horizontal position of the diaphragm pulls in the lower ribs during inspiration
• Decreased hepatic and cardiac dullness on percussion
• Signs of pulmonary hypertension (RV heave, loud P2, gallop rhythm, pansystolic
murmur, pitting pedal edema)
• Tender pulsatile liver
• Prominent v wave of jugular venous pulse
DIAGNOSIS- INVESTIGATIONS
• Spirometry:Confirmation + Assessment of severity + Follow up
assessment
• CXR
• Six minute walk test
• Pulse oximetry
• ABGs
• CT CHEST
• CBC
• ECG
21.
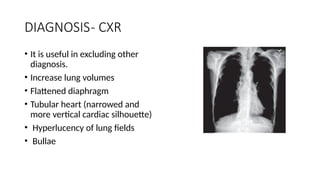
DIAGNOSIS- CXR
• Itis useful in excluding other
diagnosis.
• Increase lung volumes
• Flattened diaphragm
• Tubular heart (narrowed and
more vertical cardiac silhouette)
• Hyperlucency of lung fields
• Bullae
22.
DIAGNOSTIC TOOLS –ASSESSMENT OF
SEVERITY
The following aspects of the disease must be assessed separately.
• The presence and severity of spirometric abnormality
• Current severity of symptoms
• History of exacerbations and future risk
• Presence of co-morbidities
23.
DIAGNOSTIC TOOLS –ASSESSMENT OF
SEVERITY
• Spirometric classification of severity of COPD
• mMRC Dyspnea scale
• Combined Assessment Test (CAT Score)
• ABCD TOOL
24.
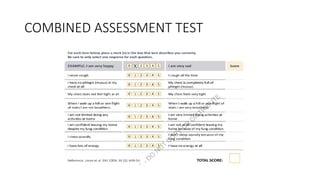
CURRENT SEVERITY OFSYMPTOMS
• Breathlessness being the cardinal symptom of the disease, one tool to
assess severity of symptoms is mMRC dyspnea scale.
• But as a matter of fact COPD impacts patients beyond just dyspnea.
So combined assessment test (CAT) can be used to measure health
status in COPD.
HISTORY OF EXACERBATIONAND FUTURE
RISK
COPD exacerbation is defined as:
• “An acute worsening of respiratory symptoms that require additional
therapy.”
28.
HISTORY OF EXACERBATIONAND FUTURE
RISK
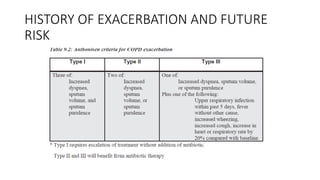
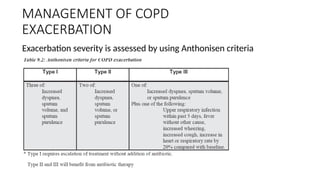
• In 1987 Anthonisen gave the classic definition
• Describing three levels of exacerbation based on patient’s
symptomatology.
• This is the criteria recommended to be used in describing the
exacerbations.
• It is used to decide the need ofantibiotic therapy.
HISTORY OF EXACERBATIONAND FUTURE
RISK
PREDICTORS OF FUTURE EXACERBATIONS RISK
• Two or more exacerbations in the past year
• History of hospitalization due to COPD in the past year
• Severe COPD, equivalent to GOLD 3 or 4
• Increased blood eosinophil count
• Use of LABA alone
• Non compliance to treatment
32.
ASSESSMENT OF COMORBIDS
COPDis a systemic disease. These conditions can increase the risk of
hospitalizations and mortality in COPD. So co-morbid illnesses should
be looked for and treated promptly.
33.
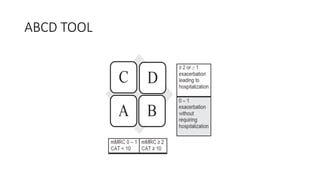
ABCD TOOL
• TheGlobal Initiative for Chronic Obstructive Lung Disease (GOLD)
ABCD assessment tool is used to classify COPD patients into four
groups (A, B, C, D) based on symptom burden, exacerbation risk and
spirometry to guide personalized treatment.
• It helps clinicians tailor therapy such as choosing long acting
bronchodilators for high risk patients (C/D)
34.
ABCD TOOL
KEY COMPONENTSOF ABCD TOOL
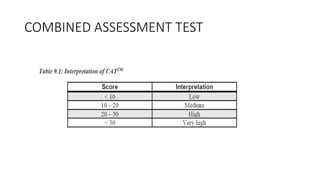
• Symptoms: Assessed using the COPD Assessment Test (CAT) or modified Medical Research Council (mMRC)
scale.
• Exacerbation History: Frequency of exacerbations and hospitalizations in the past year.
Categories:
• Group A: Low symptom burden, low risk (0-1 moderate exacerbations, no hospitalizations).
• Group B: High symptom burden, low risk.
• Group C: Low symptom burden, high risk (≥ 2 moderate exacerbation or ≥ 1 hospitalizations).
• Group D: High symptom burden, high risk.
Transition to ABE: Newer guidelines have begun shifting to an "ABE" classification for better treatment targeting.
ABE TOOL
KEY COMPONENTSOF ABE TOOL
• Symptoms: Assessed using the COPD Assessment Test (CAT) or modified Medical Research Council (mMRC)
scale.
• Exacerbation History: Frequency of exacerbations and hospitalizations in the past year.
CATEGORIES
• Group A: Low symptom burden, low risk (0-1 moderate exacerbations, no hospitalizations).
• Group B: High symptom burden, low risk.
• Group E: Any symptom level, high risk (≥ 2 moderate exacerbation or ≥ 1 hospitalizations).
37.
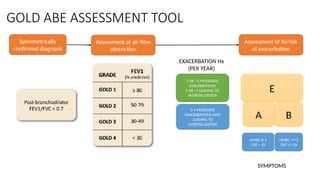
GOLD ABE ASSESSMENTTOOL
E
A B
mMRC 0-1
CAT < 10
mMRC >/=2
CAT >/=10
SYMPTOMS
2 OR >2 MODERATE
EXACERBATIONS
1 OR >1 LEADING TO
HOSPITALIZATION
0-1 MODERATE
EXACERBATIONS (NOT
LEADING TO
HOSPITALIZATION
Spirometrically
confirmed diagnosis
Assessment of air flow
obstriction
Assessment of Sx/risk
of exacerbation
EXACERBATION Hx
(PER YEAR)
38.
DIFFERENTIAL DIAGNOSIS
The maindifferential diagnosis includes:
• Asthma
• Bronchiectasis
• Tuberculosis and post-tuberculosis sequelae
• Heart failure
• Interstitial lung diseases
A careful history, clinical examination, and investigations can help rule out these
close mimics ofCOPD.
39.
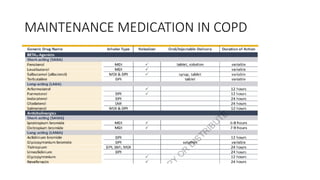
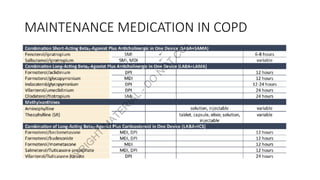
MANAGEMENT OF STABLECOPD
Bronchodilators are first line therapy for COPD.
Pharmacologic management can reduce symptoms, improve exercise
capacity, reduce the risk of exacerbations, improve overall health status
and reduce mortality.
MANAGEMENT OF STABLECOPD
KEY POINTS
• Choice of inhaler device should be tailored individually (depending on access, cost,
prescriber, patient’s preference and ability.
• Teach inhaler technique technique and recheck on each visit.
• Check inhaler technique and compliance before changing medicines.
• Inhaled bronchodilators are preferred over oral.
• Theophylline is not recommended unless other long acting treatment bronchodilators
are not available or are unaffordable.
• Long term monotherapy with ICS is not recommended.
• Long term therapy with OCS is not recommended.
MANAGEMENT OF COPD
EXACERBATION
Treatmentfor AECOPD treated at home
• Add or increase dose of bronchodilator, metered dose inhalers are preferred with spacer
device. Dose of salbutamol is 2 puff hourly (100 mg/puff) then 3 – 4 hourly. Ipratropium
bromide 2 puff 4 hourly (20 – 40 mg) can be added.
• If response is not adequate add 200 – 400 mg twice daily of sustained release theophylline.
• Add antibiotic if any evidence of infection. Amoxicillin ± clavulanate can be a good first line
option. Other antimicrobials that can be used are respiratory quinolones and macrolides.
• Oral steroids are not recommended in mild exacerbations but can be prescribed for more
severe symptoms and the dose is 30mg/day for one week.
GOALS FOR TREATMENTOF STABLE COPD
REDUCE
SYMPTOMS
• Relieve Sx
• Improve exercise tolerance
• Improve health status
REDUCE
RISK
• Prevent disease progression
• Prevent and treat exacerbations
• Reduce mortality
50.
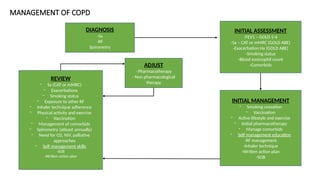
MANAGEMENT OF COPD
DIAGNOSIS
-Sx
-RF
Spirometry
INITIALASSESSMENT
-FEV1 – GOLD 1-4
-Sx – CAT or mMRC (GOLD ABE)
-Exacerbation Hx (GOLD ABE)
-Smoking status
-Blood eosinophil count
-Comorbids
INITIAL MANAGEMENT
- Smoking cessation
- Vaccination
- Active lifestyle and exercise
- Initial pharmacotherapy
- Manage comorbids
- Self management education
-RF management
-Inhaler technique
-Written action plan
-SOB
REVIEW
- Sx (CAT or mMRC)
- Exacerbations
- Smoking status
- Exposure to other RF
- Inhaler technique adherence
- Physical activity and exercise
- Vaccination
- Management of comorbids
- Spirometry (atleast annually)
- Need for O2, NIV, palliative
approaches
- Self management skills
-SOB
-Written action plan
ADJUST
- Pharmacotherapy
- Non pharmacological
therapy
51.
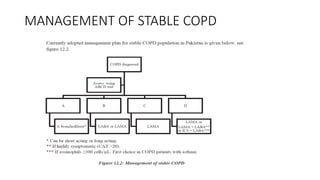
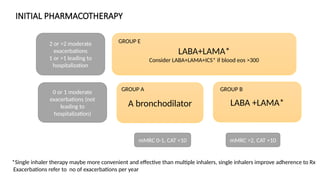
INITIAL PHARMACOTHERAPY
LABA+LAMA*
Consider LABA+LAMA+ICS*if blood eos >300
LABA +LAMA*
A bronchodilator
2 or >2 moderate
exacerbations
1 or >1 leading to
hospitalization
0 or 1 moderate
exacerbations (not
leading to
hospitalization)
mMRC 0-1, CAT <10 mMRC >2, CAT >10
GROUP E
GROUP A GROUP B
*Single inhaler therapy maybe more convenient and effective than multiple inhalers, single inhalers improve adherence to Rx
Exacerbations refer to no of exacerbations per year
52.
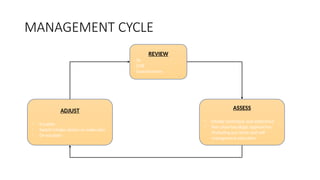
MANAGEMENT CYCLE
REVIEW
- Sx
-SOB
- Exacerbations
ASSESS
- Inhaler technique and adherence
- Non pharmacologic approaches
(Including pul rehab and self
management education
ADJUST
- Escalate
- Switch inhaler device or molecules
- De-escalate
53.
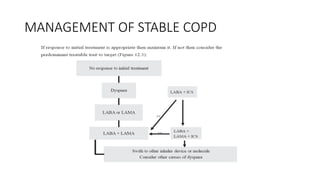
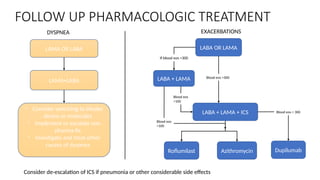
FOLLOW UP PHARMACOLOGICTREATMENT
LAMA OR LABA
LAMA+LABA
- Consider switching to inhaler
device or molecules
- Implement or escalate non
pharma Rx
- Investigate and treat other
causes of dyspnea
LABA OR LAMA
LABA + LAMA
LABA + LAMA + ICS
Roflumilast Azithromycin Dupilumab
DYSPNEA EXACERBATIONS
Blood eos >300
If blood eos <300
Blood eos
<100
Blood eos
>100
Blood eos > 300
Consider de-escalation of ICS if pneumonia or other considerable side effects
54.
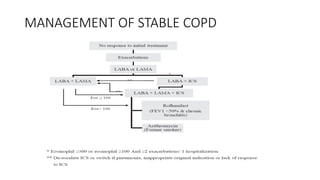
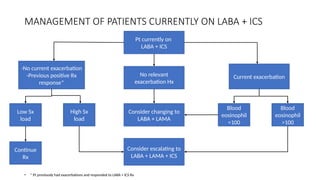
MANAGEMENT OF PATIENTSCURRENTLY ON LABA + ICS
• * Pt previously had exacerbations and responded to LABA + ICS Rx
Pt currently on
LABA + ICS
No relevant
exacerbation Hx
Consider changing to
LABA + LAMA
Consider escalating to
LABA + LAMA + ICS
-No current exacerbation
-Previous positive Rx
response*
Current exacerbation
Low Sx
load
High Sx
load
Blood
eosinophil
>100
Blood
eosinophil
<100
Continue
Rx
55.
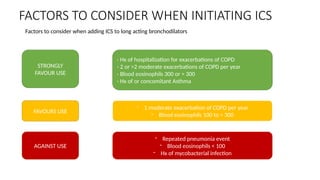
FACTORS TO CONSIDERWHEN INITIATING ICS
- Hx of hospitalization for exacerbations of COPD
- 2 or >2 moderate exacerbations of COPD per year
- Blood eosinophils 300 or > 300
- Hx of or concomitant Asthma
- 1 moderate exacerbation of COPD per year
- Blood eosinophils 100 to < 300
- Repeated pneumonia event
- Blood eosinophils < 100
- Hx of mycobacterial infection
STRONGLY
FAVOUR USE
FAVOURS USE
AGAINST USE
Factors to consider when adding ICS to long acting bronchodilators
56.
GLUCOCORTICOIDS IN COPD
•Oral steroids should be avoided if possible in stable COPD.
• Systemic steroids may be used for short-term treatment (7-14 days)
during exacerbations.
• Inhaled corticosteroids (ICS) have modest bronchodilator effect. They
reduce exacerbation severity and frequency.
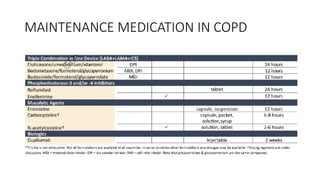
OTHER DRUGS TOAUGMENT COPD
TREATMENT
Antibiotics
• Azithromycin 250 mg/day or 500 mg three times per week for 1 year
may reduce exacerbation risk.
• Clarithromycin 250mg /day in advanced copd having bronchiectasis.
Mucolytics
• Carbocysteine and N-acetylcysteine can be used, they may reduce
exacerbations.
Antitussives
• No definite role is described for use of antitussives in COPD.
NON PHARMACOLOGIC MANAGEMENTOF
COPD
• Smoking prevention and cessation
• Control of occupational and indoor pollution
• Pulmonary rehabilitation: Exercise training, nutritional counseling,
disease education
• Vaccination: PCV (>65 yrs) and Influenza (All patients with COPD)
• Oxygen Therapy
• Non Invasive Ventilation: BiPAP
64.
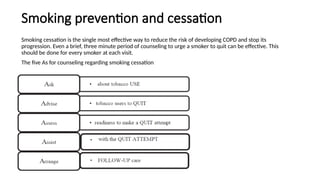
Smoking prevention andcessation
Smoking cessation is the single most effective way to reduce the risk of developing COPD and stop its
progression. Even a brief, three minute period of counseling to urge a smoker to quit can be effective. This
should be done for every smoker at each visit.
The five As for counseling regarding smoking cessation
65.
Smoking prevention andcessation
• There is a misperception of using chewable tobacco (like snuff:
naswar) or ecigarettes to help in quit attempts.
• These are not recommended and should be discouraged.
66.
Control of occupationaland indoor pollution
• Indoor pollution due to burning of wood and coal to keep houses
warm in winter and use of biomass fuel in stoves should be minimized
and measures should be taken to reduce exposure as by cooking in
open air rather than a closed kitchen, having separate cooking area,
making chimneys etc.
• Exposure to irritant particles and gases should also be avoided at
work place.
67.
Pulmonary rehabilitation
The maingoals of pulmonary rehabilitation are to increase over all
resources of the patient, to reduce handicap caused by illness or
disability and to allow integration of patient in society. This can be done
by:
• Exercise training
• Nutritional counseling
• Education
68.
Exercise training
• Inpatients with mild to moderate COPD, suitable exercises are
walking, cycling and swimming.
• Daily exercise should be done for about 30 minutes, it may be divided
into 2 – 3 phases or till the patient gets out of breath.
• In severe COPD, it should be done to improve strength and
endurance of muscles. This should involve respiratory, abdominal,
back, head, neck and limbs to improve quality of life.
69.
Nutritional counseling
• LowBMI is an independent risk factor for mortality in COPD patients.
• Increased calorie intake should be accompanied by regimens with
anabolic action.
• On the other side obese individuals have greater levels of
breathlessness and impairment of activity.
• Well-balanced diet is recommended.
70.
Education
• Educate regardingdisease, its progressive nature, smoking cessation,
drug treatment and how to manage exacerbations.