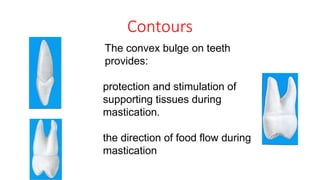
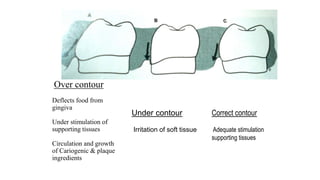
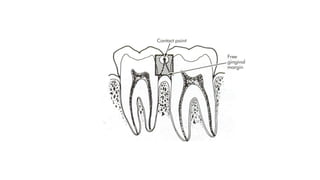
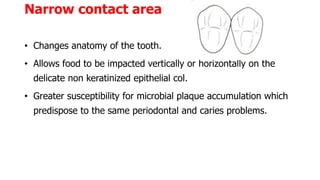
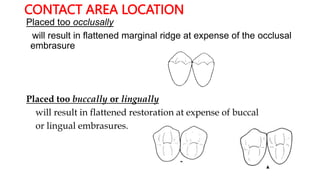
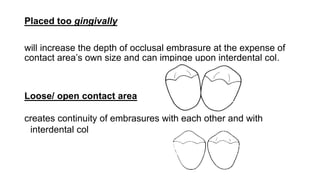
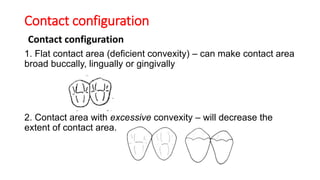
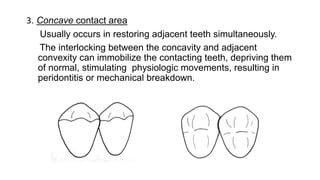
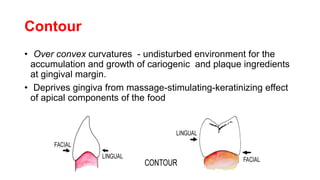
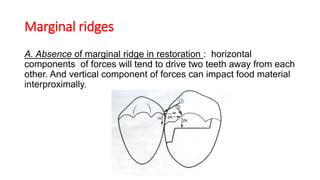
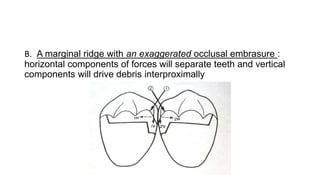
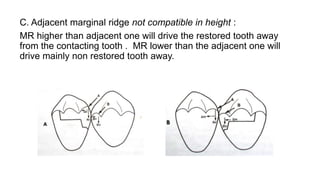
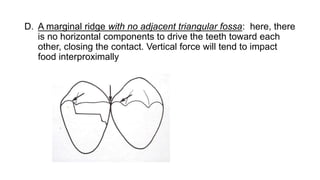
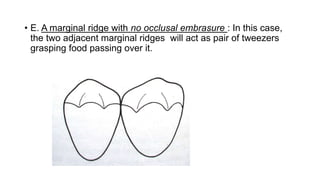
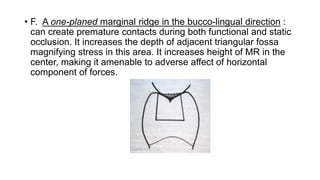
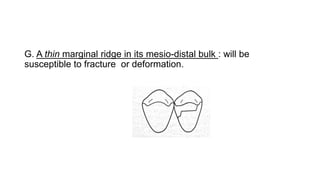
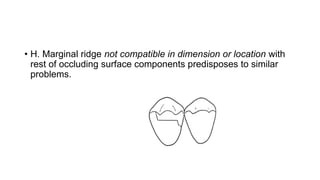
This document discusses contours, contacts, and marginal ridges in restorative dentistry. It defines these anatomical features and explains their roles in proper function and supporting tissue health. Faulty reproduction of contours, contacts, or marginal ridges can result in issues like food impaction, inflammation, and periodontal disease. Examples are given of specific faults and their potential consequences, highlighting the importance of accurately restoring these features for optimal restoration outcomes.


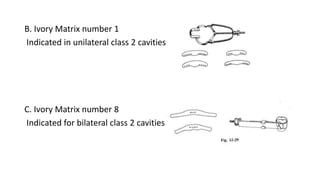


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







