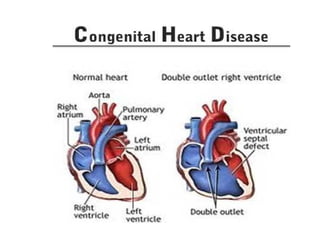
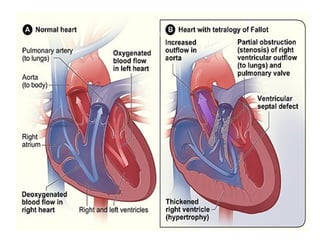
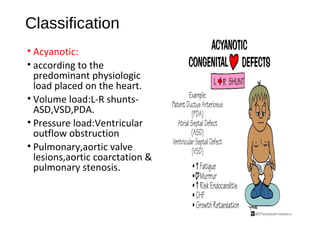
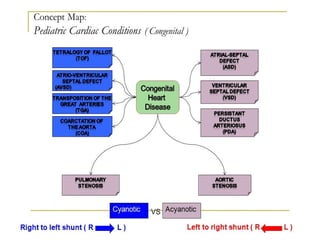
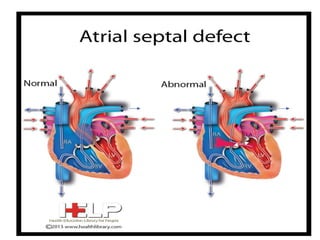
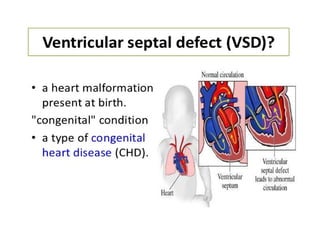
Congenital heart disease has a prevalence of 0.5-0.8% of live births. It can be caused by genetic and environmental factors. Defects are classified as acyanotic if there is increased blood flow to the lungs, or cyanotic if there is decreased pulmonary blood flow. Common defects include atrial septal defects, ventricular septal defects, and patent ductus arteriosus. Diagnosis involves tests like echocardiogram and chest x-ray. Treatment options include procedures to close defects, heart transplantation, open heart surgery, and medications to manage symptoms.