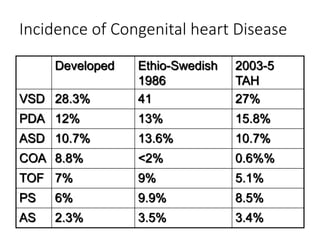
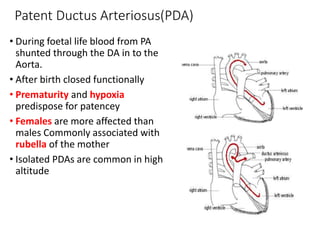
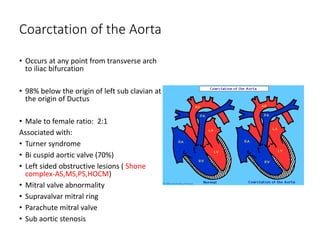
This document discusses congenital heart diseases, beginning with a review of fetal circulation and how it transitions after birth. It then classifies common acyanotic and cyanotic congenital heart diseases. Ventricular septal defect, patent ductus arteriosus, and coarctation of the aorta are discussed in more detail, including their pathophysiology, clinical presentation, diagnosis, and management principles. The objective is to revise fetal circulation, classify congenital heart diseases, and discuss common types and their clinical approach.