Download to read offline


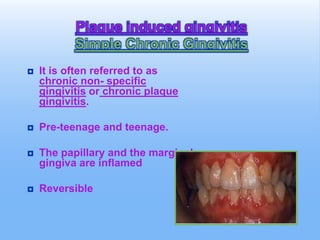

















This document discusses chronic and conditioned gingival overgrowth in children. It covers several topics: 1. Plaque-induced gingivitis including simple chronic gingivitis and conditional gingival enlargement due to hormonal changes, drugs like Dilantin, and nutritional deficiencies. 2. Genetic causes of gingival overgrowth like gingival fibromatosis. 3. Specific conditions are described in more detail such as puberty gingivitis, Dilantin-induced gingival hyperplasia, and scorbutic gingivitis. Treatment options and complications are provided.










































































