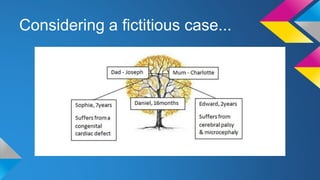
The document discusses the complications of prematurity, including definitions, causes, acute and chronic effects, and prevention strategies. It highlights a case study of a 16-month-old child with severe complications including bronchopulmonary dysplasia and developmental delays. Possible predictors and preventive measures, such as the use of antibiotics and cervical cerclage, are also covered.