3
INTRODUCTION
Derived from thegreek word “ kolla” – “glue” and gen- “
producing.”
In French “collagene” means glue producing constraints as
collagen tissues were used as glue and gelatin.
Miller and Matukas discovered collagen in 1969, since then
around 28 new collagen types have been found.
Most abundant protein in mammals -1/3rd of total protein,
3/4th of the dry weight of skin and is the most prevalent
component of extracellular matrix.
4.
4
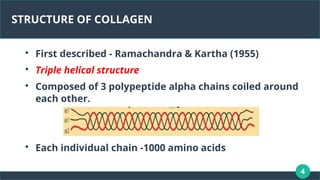
STRUCTURE OF COLLAGEN
Firstdescribed - Ramachandra & Kartha (1955)
Triple helical structure
Composed of 3 polypeptide alpha chains coiled around
each other.
Each individual chain -1000 amino acids
5.
5
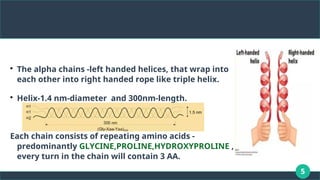
The alpha chains-left handed helices, that wrap into
each other into right handed rope like triple helix.
Helix-1.4 nm-diameter and 300nm-length.
Each chain consists of repeating amino acids -
predominantly GLYCINE,PROLINE,HYDROXYPROLINE ,
every turn in the chain will contain 3 AA.
6.
6
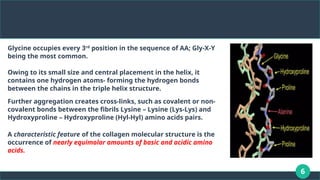
Glycine occupies every3rd
position in the sequence of AA; Gly-X-Y
being the most common.
Owing to its small size and central placement in the helix, it
contains one hydrogen atoms- forming the hydrogen bonds
between the chains in the triple helix structure.
Further aggregation creates cross-links, such as covalent or non-
covalent bonds between the fibrils Lysine – Lysine (Lys-Lys) and
Hydroxyproline – Hydroxyproline (Hyl-Hyl) amino acids pairs.
A characteristic feature of the collagen molecular structure is the
occurrence of nearly equimolar amounts of basic and acidic amino
acids.
7.
7
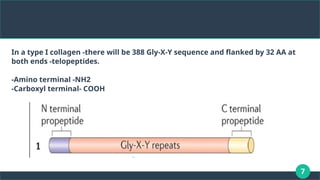
In a typeI collagen -there will be 388 Gly-X-Y sequence and flanked by 32 AA at
both ends -telopeptides.
-Amino terminal -NH2
-Carboxyl terminal- COOH
9
BIOSYNTHESIS OF COLLAGENFIBRE
GENE EXPRESSION
TRANSLATION AND POST-TRANSLATION EVENTS (INTRACELLULAR
EVENTS)
EXTRACELLULAR COLLAGEN BIOSYNTHESIS
REGULATION OF SYNTHESIS
10.
10
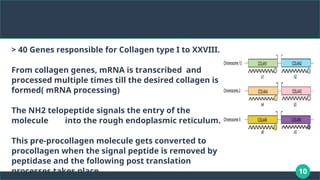
> 40 Genesresponsible for Collagen type I to XXVIII.
From collagen genes, mRNA is transcribed and
processed multiple times till the desired collagen is
formed( mRNA processing)
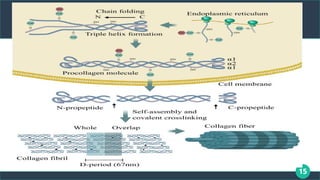
The NH2 telopeptide signals the entry of the
molecule into the rough endoplasmic reticulum.
This pre-procollagen molecule gets converted to
procollagen when the signal peptide is removed by
peptidase and the following post translation
processes takes place.
11.
11
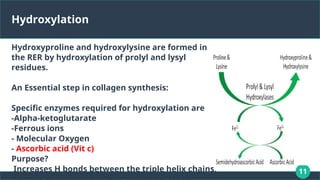
Hydroxylation
Hydroxyproline and hydroxylysineare formed in
the RER by hydroxylation of prolyl and lysyl
residues.
An Essential step in collagen synthesis:
Specific enzymes required for hydroxylation are
-Alpha-ketoglutarate
-Ferrous ions
- Molecular Oxygen
- Ascorbic acid (Vit c)
Purpose?
Increases H bonds between the triple helix chains,
12.
12
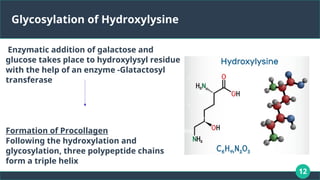
Glycosylation of Hydroxylysine
Enzymaticaddition of galactose and
glucose takes place to hydroxylysyl residue
with the help of an enzyme -Glatactosyl
transferase
Formation of Procollagen
Following the hydroxylation and
glycosylation, three polypeptide chains
form a triple helix
13.
13
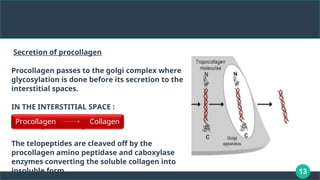
Secretion of procollagen
Procollagenpasses to the golgi complex where
glycosylation is done before its secretion to the
interstitial spaces.
IN THE INTERSTITIAL SPACE :
Procollagen collagen
→
The telopeptides are cleaved off by the
procollagen amino peptidase and caboxylase
enzymes converting the soluble collagen into
insoluble form.
Procollagen Collagen
14.
14
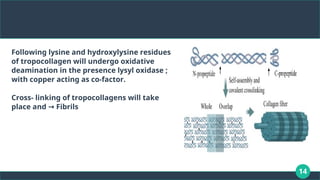
Following lysine andhydroxylysine residues
of tropocollagen will undergo oxidative
deamination in the presence lysyl oxidase ;
with copper acting as co-factor.
Cross- linking of tropocollagens will take
place and Fibrils
→
16
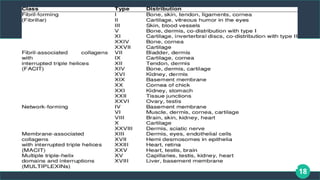
Types of collagen
29types present
Depending on variations brought by
Assembly of polypeptide chains
Different lengths of helix
Various interruptions in helix
Difference in terminations of helical domains; they can be divided into:
1. Fibril forming collagens
2.FACIT collagens
3.Non-Fibrillar collagens
17.
17
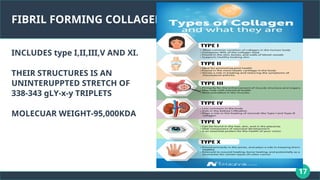
FIBRIL FORMING COLLAGENS
INCLUDEStype I,II,III,V AND XI.
THEIR STRUCTURES IS AN
UNINTERUPPTED STRETCH OF
338-343 gLY-x-y TRIPLETS
MOLECUAR WEIGHT-95,000KDA
19
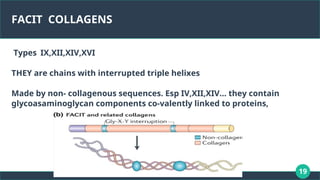
FACIT COLLAGENS
Types IX,XII,XIV,XVI
THEYare chains with interrupted triple helixes
Made by non- collagenous sequences. Esp IV,XII,XIV… they contain
glycoasaminoglycan components co-valently linked to proteins,
20.
20
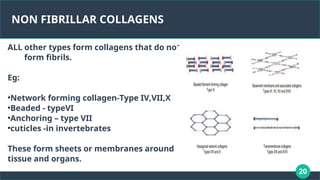
NON FIBRILLAR COLLAGENS
ALLother types form collagens that do not
form fibrils.
Eg:
•Network forming collagen-Type IV,VII,X
•Beaded - typeVI
•Anchoring – type VII
•cuticles -in invertebrates
These form sheets or membranes around
tissue and organs.
21.
21
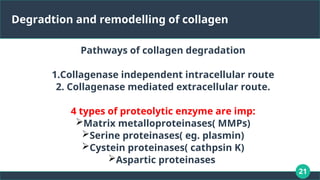
Degradtion and remodellingof collagen
Pathways of collagen degradation
1.Collagenase independent intracellular route
2. Collagenase mediated extracellular route.
4 types of proteolytic enzyme are imp:
Matrix metalloproteinases( MMPs)
Serine proteinases( eg. plasmin)
Cystein proteinases( cathpsin K)
Aspartic proteinases
22.
22
MMPs are essentialfor degradation
2 Main mechanisms involved:
1)Extracellular degradation by enzymes :
Fibroblasts , PMNLs, macrophages secrete collagenases + enzymes =
MMPS. MMPs are zinc –containing enzymes secreted as inactive
precursors and regulated by cytokines ( IL-1) .
They are inhibited by TIMPs ; secreted by fibroblasts and macrophages.
24.
2) Intracellular degradationby phagocytosis :
Fibroblasts phagocytose collagen fibers, degrading collagen at
specific interfaces such as ligament–cementum, without the
involvement of MMPs. This pathway utilizes lysosomal
enzymes that operate in acidic environments.
Regulation of MMP activity by inhibitors like TIMPs is crucial for
maintaining tissue homeostasis. Moreover, factors like
glucocorticoids and retinoids can inhibit MMP production and
increase TIMP production, balancing collagen degradation
processes.
26.
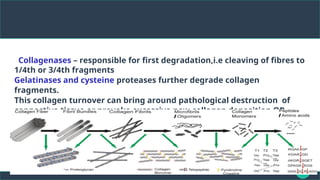
eCollagenases – responsiblefor first degradation,i.e cleaving of fibres to
1/4th or 3/4th fragments
Gelatinases and cysteine proteases further degrade collagen
fragments.
This collagen turnover can bring around pathological destruction of
connective tissue or provoke excessive new collagen deposition OR
fibrosis.
struction of connective tissue or provoke excessive new collagen deposition and
fibrosis,
27.
27
They do nothave substrate specificity as host
collagenase.
MMPs show strict substrate specificity for collagen
hydrolysis, cleaving collagen only at well-defined
recognition
sites.
However, BACTERIAL collagenases have
no obvious preference for any type of collagen and
can
hydrolyze collagen in multiple locations and
completely
decompose it into small peptides.
28.
28
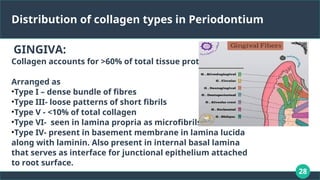
Distribution of collagentypes in Periodontium
GINGIVA:
Collagen accounts for >60% of total tissue protein.
Arranged as
•Type I – dense bundle of fibres
•Type III- loose patterns of short fibrils
•Type V - <10% of total collagen
•Type VI- seen in lamina propria as microfibrils
•Type IV- present in basement membrane in lamina lucida
along with laminin. Also present in internal basal lamina
that serves as interface for junctional epithelium attached
to root surface.
29.
29
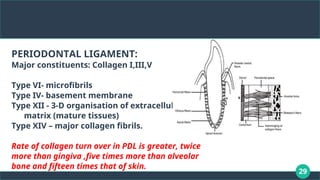
PERIODONTAL LIGAMENT:
Major constituents:Collagen I,III,V
Type VI- microfibrils
Type IV- basement membrane
Type XII - 3-D organisation of extracellular
matrix (mature tissues)
Type XIV – major collagen fibrils.
Rate of collagen turn over in PDL is greater, twice
more than gingiva ,five times more than alveolar
bone and fifteen times that of skin.
30.
30
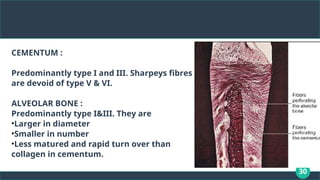
CEMENTUM :
Predominantly typeI and III. Sharpeys fibres
are devoid of type V & VI.
ALVEOLAR BONE :
Predominantly type I&III. They are
•Larger in diameter
•Smaller in number
•Less matured and rapid turn over than
collagen in cementum.
31.
31
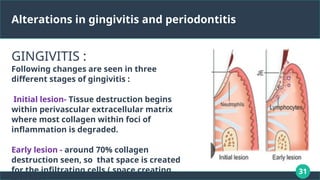
Alterations in gingivitisand periodontitis
GINGIVITIS :
Following changes are seen in three
different stages of gingivitis :
Initial lesion- Tissue destruction begins
within perivascular extracellular matrix
where most collagen within foci of
inflammation is degraded.
Early lesion - around 70% collagen
destruction seen, so that space is created
for the infiltrating cells.( space creating
32.
32
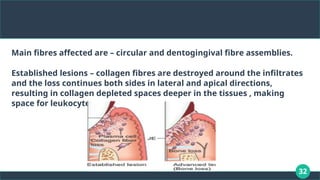
Main fibres affectedare – circular and dentogingival fibre assemblies.
Established lesions – collagen fibres are destroyed around the infiltrates
and the loss continues both sides in lateral and apical directions,
resulting in collagen depleted spaces deeper in the tissues , making
space for leukocyte infiltration
33.
33
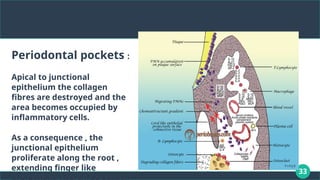
Periodontal pockets :
Apicalto junctional
epithelium the collagen
fibres are destroyed and the
area becomes occupied by
inflammatory cells.
As a consequence , the
junctional epithelium
proliferate along the root ,
extending finger like
34.
34
Uses of collagenin periodontics
DRUG Delivery
Key benefit- high concentration of
drug can be delivered and
localized in the target site .
Avoid risk of systemic toxicity and
their side effects.
Drugs are loaded into the collagen
membranes by H bonds, covalent
or simple entrapment.
35.
35
Tissue augmentation andrecession
coverage
Collagen membranes used as an alternative in
mucogingival surgeries
Shows similar histologic and clinical
outcomes, also achieving complete root
coverages.
Gets completely incorporated in adjacent host
connective tissues with less signs of
inflammation.
36.
36
Bone substitute –bone grafts in intra
bony defects:
Collagen has bone inducing proteins
Osteo-inductive activity.
Demineralized bone collagen is used as
bone graft material for treatment of
acquired and congenital bone defects by
itself or in combination with
hydroxyapatite crystals.
38
Guided tissue regeneration– GTR
membranes
GTR – reconstitutes lost tissues and based
on selective repopulation,
Reported initially by Neyman et al (1982)
And later coined by Gottlow et al (1986).
GTR includes adding a barrier to prevent
the fast growing cells from migration to
the wound site.
40
Hemostat:
During blood clotting, platelets become
activated by thrombin and aggregate at
injury site.
When stimulated by protein fibrinogen , the
platelets adhere tp he collagen by
clumping .
Collagen is a natural hemostat and a wide
variety of collagen based products are used
to control excessive bleeding.
42
Diseases associated withcollagen alterations:
Broadly classified as
3 Types of alterations can affect collagens and lead to connective tissue
changes :
1. Defect in structure of collagen genes
2. Molecular defect in processing enzymes
3.Mechanisms affecting expression of collagen genes due to pathologies
of acquired diseases.
1. Inherited diseases
2. Acquired diseases
43.
43
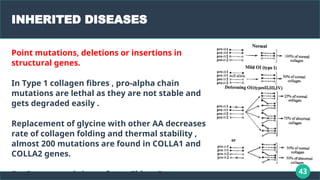
INHERITED DISEASES
Point mutations,deletions or insertions in
structural genes.
In Type 1 collagen fibres , pro-alpha chain
mutations are lethal as they are not stable and
gets degraded easily .
Replacement of glycine with other AA decreases
rate of collagen folding and thermal stability ,
almost 200 mutations are found in COLLA1 and
COLLA2 genes.
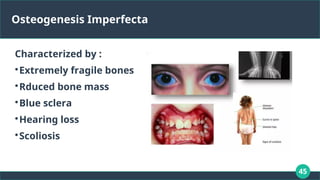
Eg: Osteogenesis imperfecta. Ehlers Danos
44.
44
ACQUIRED DISEASES
Morecommon
Gene expression affected rather
than gene structure.
Eg Chronic inflammatory diseases
like Rheumatoid Arthritis, chronic
periodontitis, Sjogrens disease and
fibrosed conditions like
atherosclerosis , pulmonary fibrosis
etc.
46
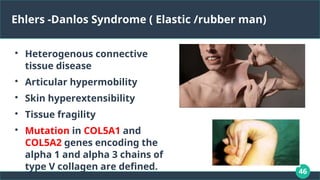
Ehlers -Danlos Syndrome( Elastic /rubber man)
Heterogenous connective
tissue disease
Articular hypermobility
Skin hyperextensibility
Tissue fragility
Mutation in COL5A1 and
COL5A2 genes encoding the
alpha 1 and alpha 3 chains of
type V collagen are defined.
47.
47
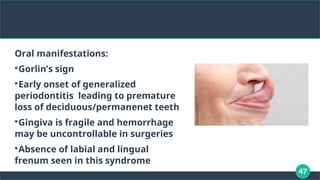
Oral manifestations:
Gorlin’s sign
Earlyonset of generalized
periodontitis leading to premature
loss of deciduous/permanenet teeth
Gingiva is fragile and hemorrhage
may be uncontrollable in surgeries
Absence of labial and lingual
frenum seen in this syndrome
48.
48
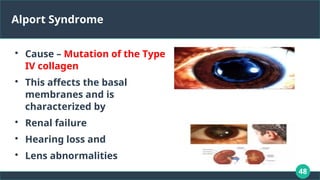
Alport Syndrome
Cause –Mutation of the Type
IV collagen
This affects the basal
membranes and is
characterized by
Renal failure
Hearing loss and
Lens abnormalities
49.
49
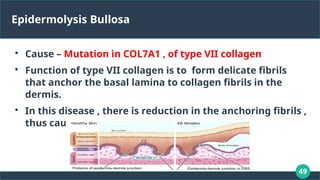
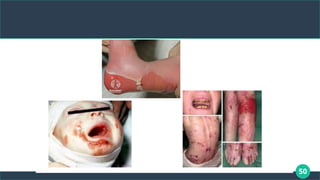
Epidermolysis Bullosa
Cause –Mutation in COL7A1 , of type VII collagen
Function of type VII collagen is to form delicate fibrils
that anchor the basal lamina to collagen fibrils in the
dermis.
In this disease , there is reduction in the anchoring fibrils ,
thus causing friction and blistering.
51
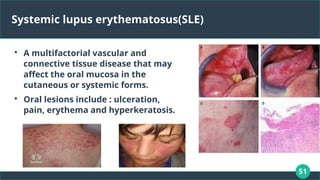
Systemic lupus erythematosus(SLE)
Amultifactorial vascular and
connective tissue disease that may
affect the oral mucosa in the
cutaneous or systemic forms.
Oral lesions include : ulceration,
pain, erythema and hyperkeratosis.
52.
52
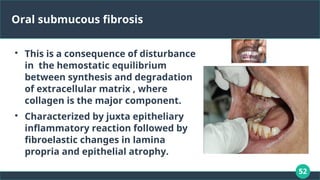
Oral submucous fibrosis
Thisis a consequence of disturbance
in the hemostatic equilibrium
between synthesis and degradation
of extracellular matrix , where
collagen is the major component.
Characterized by juxta epitheliary
inflammatory reaction followed by
fibroelastic changes in lamina
propria and epithelial atrophy.
53.
53
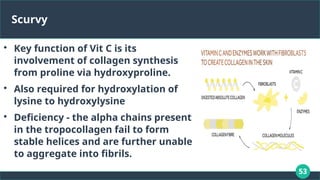
Scurvy
Key function ofVit C is its
involvement of collagen synthesis
from proline via hydroxyproline.
Also required for hydroxylation of
lysine to hydroxylysine
Deficiency - the alpha chains present
in the tropocollagen fail to form
stable helices and are further unable
to aggregate into fibrils.
54.
54
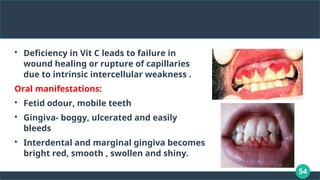
Deficiency in VitC leads to failure in
wound healing or rupture of capillaries
due to intrinsic intercellular weakness .
Oral manifestations:
Fetid odour, mobile teeth
Gingiva- boggy, ulcerated and easily
bleeds
Interdental and marginal gingiva becomes
bright red, smooth , swollen and shiny.
55.
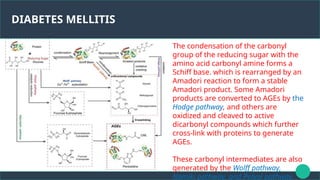
DIABETES MELLITIS
The condensationof the carbonyl
group of the reducing sugar with the
amino acid carbonyl amine forms a
Schiff base. which is rearranged by an
Amadori reaction to form a stable
Amadori product. Some Amadori
products are converted to AGEs by the
Hodge pathway, and others are
oxidized and cleaved to active
dicarbonyl compounds which further
cross-link with proteins to generate
AGEs.
These carbonyl intermediates are also
generated by the Wolff pathway,
Namiki pathway, and Polyol pathway.
56.
56
Diabetes Mellitis( metabolicdisorder)
In the hyperglycemic state , numerous proteins and
matrix molecules undergoes non-enzymatic glycosylation,
resulting in advanced glycation end products (AGEs).
Collagen gets crosslinked with these AGEs making it less
soluble and less likely for any repair/replacement.
As a result in poorly controlled diabetes patients collagen
is aged and more susceptible to breakdown, ie. easily
destroyed by infections.
57.
57
Gingival enlargements
1. HereditaryGingival enlargements:
Both in dominant and recessive autosomal inheritance.
Is a gradual progressive benign enlargement that affects
marginal, attached and interdental gingiva.
Histopathologically it shows increase in both extracellular
matrix and cell numbers.
58.
58
2. Drug inducedenlargements
a} Phenytoin :
Fibroblasts becomes sensitive to this drug- increase in
collagen production.
The collagenase produced by these phenytoin sensitive
fibrea are relatively inactive to degrade collagen
This imbalance results in overacculmulation of colllagen
and increase in connective tissue
59.
59
B} Calcium channelblockers like nifedipine interact with the gingival
fibroblast aleading to overproduction of collagen and increase in
gingival size
C} Cyclosporin
they were found to react with a phenotypically distinct subpopulation of
gingival fibroblasts to enhance protein synthesis.
60.
60
CONCLUSION
Collagen serve importantmechanical and structural
support within the body, especially in connective tissues
and also exerts their value in cellular microenviornment.
Knowledge of the structure , biosynthesis and interaction
with other components plays an important role in the
understanding of its function in the periodontium.
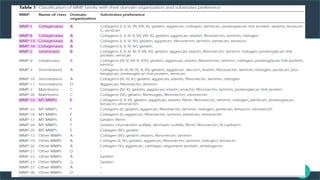
#24 MMPs are a family of proteolytic enzymes that have different substrate preferences, while share the same zinc-dependent active site and have similar structural features [27]. They are grouped into collagenases, gelatinases, stromelysins, matrilysins and membrane-type (MT)MMPs and others, which are characterized by their domain organization and substrate preference (
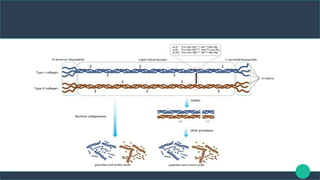
#26 Schematic model for stepwise collagen degradation by the S8 protease myroicolsin from Myroides profundi D25. Black arrows indicate the collagenolytic process of myroicolsin from collagen fiber to peptides and amino acids. Green arrows indicate the cross-links or bonds destroyed by myroicolsin in each step. Red arrows indicate the cleavage sites of myroicolsin on synthetic peptides. T1, T2, and T3 are the three polypeptide chains in a collagen monomer, and dotted lines indicate the hydrogen bonds between the polypeptide chains in a collagen monomer