MAXILLOMANDIULAR RELATIONS ANDRECORD
MAXILLOMANDIBULAR RELATIONSHIP:
Any spatial relationship of maxilla to the mandible;
any one of the infinite relationship of the mandible to the
maxilla (GPT8)
MAXILLOMANDIBULAR RELATONSHIP RECORD:
A registration of any positional relationship of the mandible
relative to maxilla (GPT)
4.
Maxillomandibular relations areclassified into:
1. Orientation relation
Establish the relationship of the maxilla into cranium
2. Vertical relation
Establish the degree of jaw separation or vertical height
of
the face
3. Horizontal relation
Establish the antero-posterior and side to side
relationship
5.
ORIENTATION JAW RELATION
•It is the first jaw relation to be recorded.
• It establishes the relationship of maxilla to the base of skull
or cranium.
• It establishes the angle or tilt of the maxilla in three
reference planes.
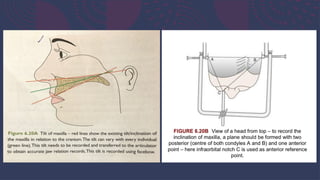
• To record the angulation of the maxilla, a plane should be
formed with atleast two posterior reference point and one
anterior reference point
7.
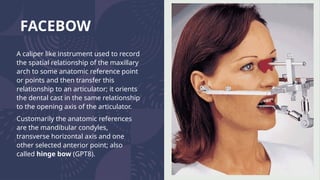
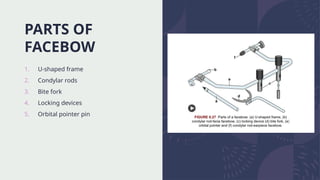
FACEBOW
A caliper likeinstrument used to record
the spatial relationship of the maxillary
arch to some anatomic reference point
or points and then transfer this
relationship to an articulator; it orients
the dental cast in the same relationship
to the opening axis of the articulator.
Customarily the anatomic references
are the mandibular condyles,
transverse horizontal axis and one
other selected anterior point; also
called hinge bow (GPT8).
8.
Types of facebow
1.Arbitraryfacebow
It determine the centre of rotation of condyle
2.Kinematic / hinge facebow
It establishes the centre accurately
9.
ARBITRARY FACEBOW
DEFINITION:
A deviceused to relate the maxillary cast to the condylar elements of an articulator using
(average anatomic landmarks to estimate the position of the transverse horizontal axis on
the face (GPI8).
• Also called 'average axis facebow’.
• It is the most commonly used facebow and is preferred for complete denture
construction.
• The hinge axis (transverse horizontal axis) is approximately located. It positions the rods
within 5 mm of the true centre of rotation of condyle.
• This method does not locate the true hinge axis, but the clinical impact of this inaccuracy
is minimal and will lead to a mild error in the occlusion, which can be adjusted during
insertion of the complete dentures.
10.
Arbitrary facebows areclassified into
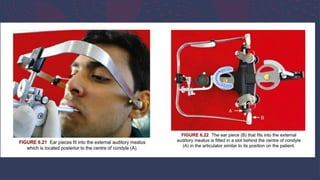
Earpiece type(ear bow):
• The external auditory meatus is considered as reference point
to determine the centre of condylar rotation.
• The condyles are located at an approximate distance in front
of the meatus and this is compensated for in the articulator by
mounting the facebow behind the condylar centre.
• This type of facebow is easier to manipulate clinically
11.
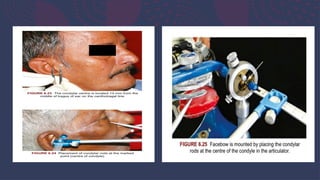
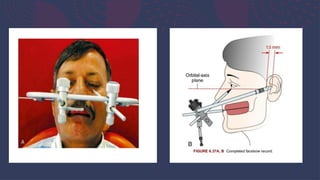
Facial type:
• Thecentre of condylar rotation is arbitrarily marked as 13
mm anterior to the middle of the tragus of the ear, on a line
drawn from the outer canthus of the eye to the middle of the
tragus of the ear - canthotragal line.
• The condylar rods of the facebow are placed on this point.
• This facebow is mounted by placing the condylar rods at the
centre of the condyle in the articulator.
14.
KINEMATIC FACEBOW
DEFINITION:
• Afacebow with adjustable caliper ends used to locate the transverse horizontal
axis of the mandible (GPT8).
• It locates the true (exact) centre of condylar rotation or transverse horizontal axis.
• It is preferred in full mouth reconstructions.
• It usually requires a fully adjustable articulator.
• When we consider the rotation of any circular object, only the central point
rotates, any other point within the circle will show translatory movement.
• Similarly in the condyle, the centre alone will display pure rotation. This principle
used to determine the true centre of rotation using kinematic facebow.
15.
• The condylarrods are first positioned arbitrarily similar to facia type
of facebow at a point 13 mm anterior to the auditory meatus on the
canthotragal line.
• The patient is instructed to make opening and closing movements in
CR. The opening should not be greater than 12 mm as then the
condyle will then begin to translate instead of rotating.
• The position of the condylar rod is shifted around the arbitrary mark
until it shows pure rotation. This is the centre of condylar rotation.
• This point is marked, the condylar rods are locked, the facebow
assembly is removed and mounted on an appropriate articulator.
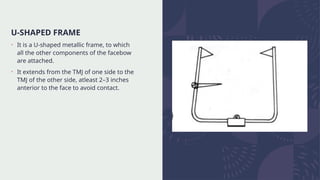
U-SHAPED FRAME
• Itis a U-shaped metallic frame, to which
all the other components of the facebow
are attached.
• It extends from the TMJ of one side to the
TMJ of the other side, atleast 2–3 inches
anterior to the face to avoid contact.
19.
CONDYLAR RODS
• Theseare two calibrated metal extensions
fitted on either side of the free end of the
U-shaped frame that are placed on the
determined centre of condyle.
• The calibrations on either side are
equalized (to centre the facebow) and
then locked.
20.
BITE FORK
• Itis a U-shaped rod which is attached to
the maxillary occlusal rim while recording
the orientation jaw relation.
• It is attached to the frame with the help
of a metal rod called the ‘stem’.
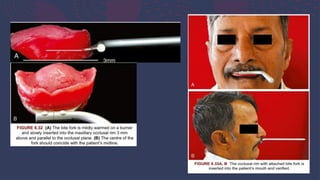
• The bite fork should be inserted about 3
mm above the occlusal surface into the
occlusal rim.
• Sometimes the bite fork is attached to
the occlusal surface of the occlusal rim
with the help of impression compound.
• This is done in order to preserve the
occlusal rim.
21.
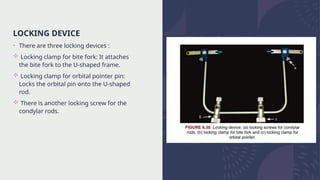
LOCKING DEVICE
• Thereare three locking devices :
Locking clamp for bite fork: It attaches
the bite fork to the U-shaped frame.
Locking clamp for orbital pointer pin:
Locks the orbital pin onto the U-shaped
rod.
There is another locking screw for the
condylar rods.
22.
ORBITAL PLANE
• Ithelps in marking the anterior reference
point.
• It is adjusted after marking the anterior
reference point on the patient.
• This enables the transfer of the third
reference point.
23.
FACEBOW TRANSFER
• Theprocedure of transferring the orientation of the maxilla
to the articulator involves:
Facebow record
Facebow mounting
24.
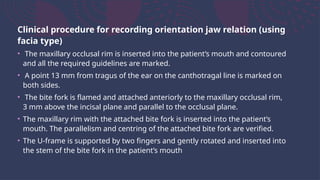
Clinical procedure forrecording orientation jaw relation (using
facia type)
• The maxillary occlusal rim is inserted into the patient’s mouth and contoured
and all the required guidelines are marked.
• A point 13 mm from tragus of the ear on the canthotragal line is marked on
both sides.
• The bite fork is flamed and attached anteriorly to the maxillary occlusal rim,
3 mm above the incisal plane and parallel to the occlusal plane.
• The maxillary rim with the attached bite fork is inserted into the patient’s
mouth. The parallelism and centring of the attached bite fork are verified.
• The U-frame is supported by two fingers and gently rotated and inserted into
the stem of the bite fork in the patient’s mouth
25.
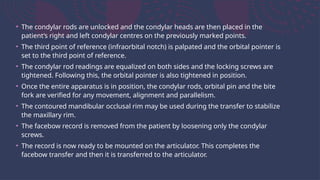
• The condylarrods are unlocked and the condylar heads are then placed in the
patient’s right and left condylar centres on the previously marked points.
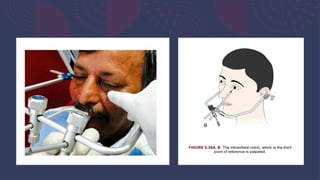
• The third point of reference (infraorbital notch) is palpated and the orbital pointer is
set to the third point of reference.
• The condylar rod readings are equalized on both sides and the locking screws are
tightened. Following this, the orbital pointer is also tightened in position.
• Once the entire apparatus is in position, the condylar rods, orbital pin and the bite
fork are verified for any movement, alignment and parallelism.
• The contoured mandibular occlusal rim may be used during the transfer to stabilize
the maxillary rim.
• The facebow record is removed from the patient by loosening only the condylar
screws.
• The record is now ready to be mounted on the articulator. This completes the
facebow transfer and then it is transferred to the articulator.
31.
Mounting on thearticulator
• The articulator is programmed first (zeroing of articulator):
• The incisal guide pin is set to correct jaw separation and the anterior stop screws are
tightened first.
• Next the horizontal condylar inclination is set at 40° and the Bennett angle at 20°.
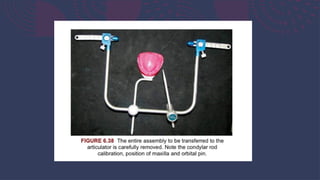
• The facebow record is now mounted on the articulator as follows:
• The condylar rods are attached to the auditory pins.
• The bite fork is stabilized on the tilting support bar provided and the orbital pin is made to
coincide with the orbital axis plane indicator.
• The incisal pin is locked with its lock screw at zero on calibration and the incisal table is set
horizontally
• The upper member of the articulator is swung open, plaster is mixed and placed on the cast
and the upper member is closed , until the incisal pin fully touches the incisal table and
upper mounting plate is covered with plaster.
• Excess plaster is trimmed once the plaster is set. Facebow is now removed by loosening all
the locking devices.
33.
INDICATIONS OF FACEBOW
•Balanced occlusion is desired.
• Vertical dimension is subject to change.
• If a facebow is not used, the maxillary cast is mounted
arbitrarily on the articulator using the occlusal plane as a
guide.
https://youtu.be/kCbHTxgwZLc?si=4zTLCA9M6_PlOplT
34.
CONCLUSION
• Failure touse the facebow may lead to errors in occlusion of the
denture. These errors depend on the orientation of casts,
interocclusal record and type of the teeth to be used.
• If cusp teeth are to be used or if the interocclusal records are made
with the teeth out of contact, facebow record becomes essential.
• Hinge axis is a component of every masticatory movement of the
mandible and therefore cannot be disregarded and this hinge axis
should be accurately captured and transferred to the articulator. So
it becomes a fine representative of the patient and biologically
acceptable restoration is possible.