Downloaded 393 times
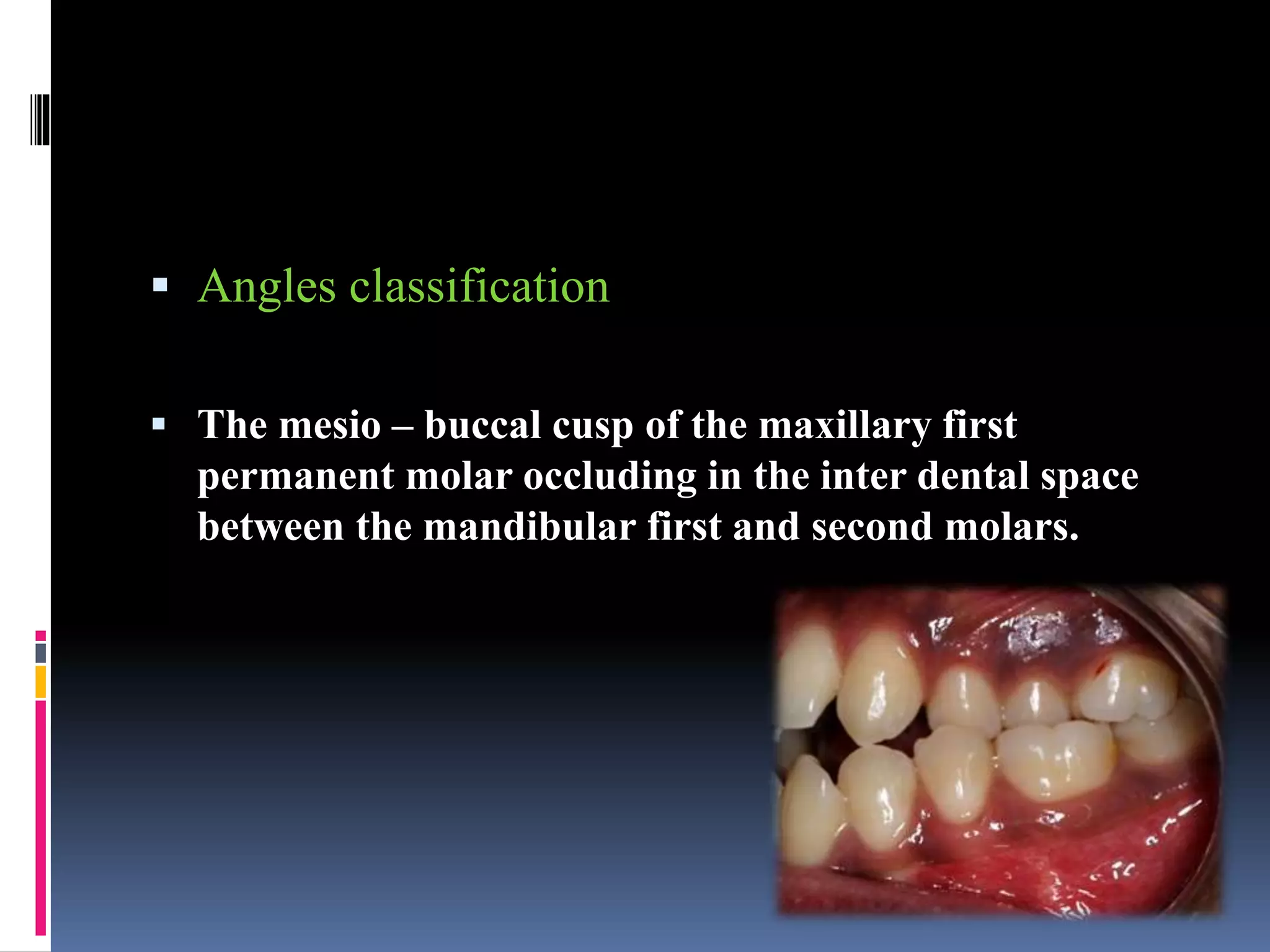


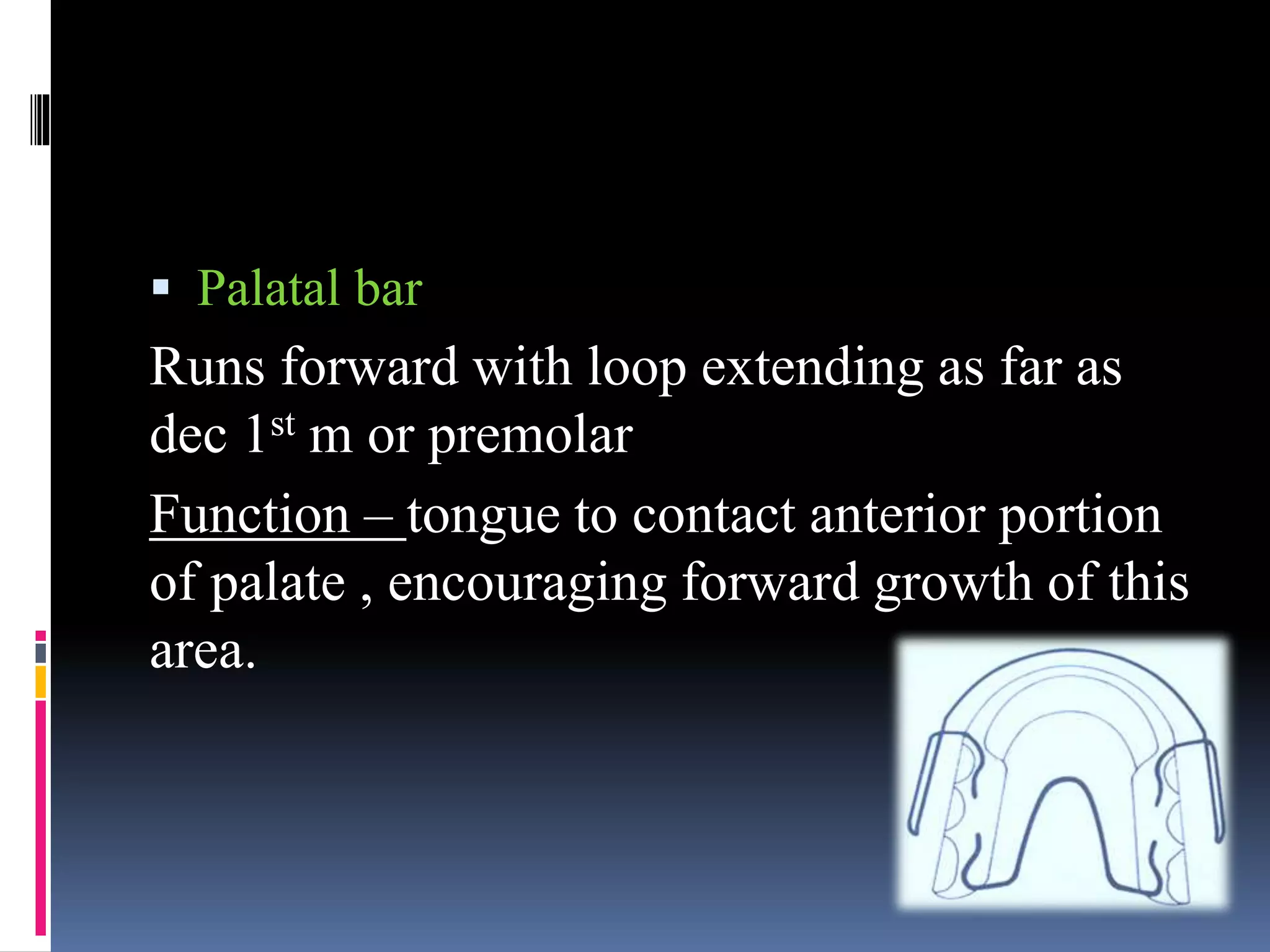
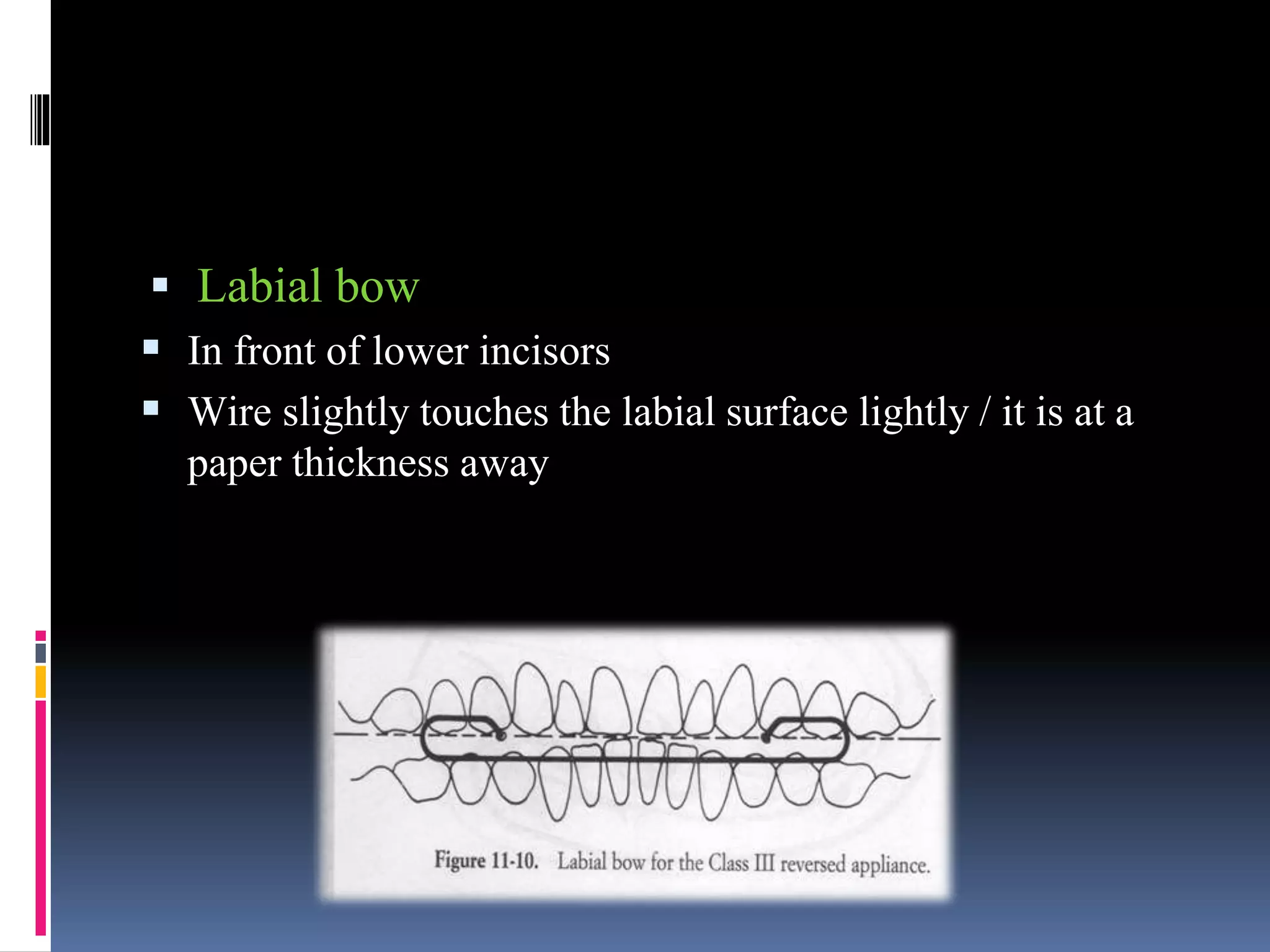

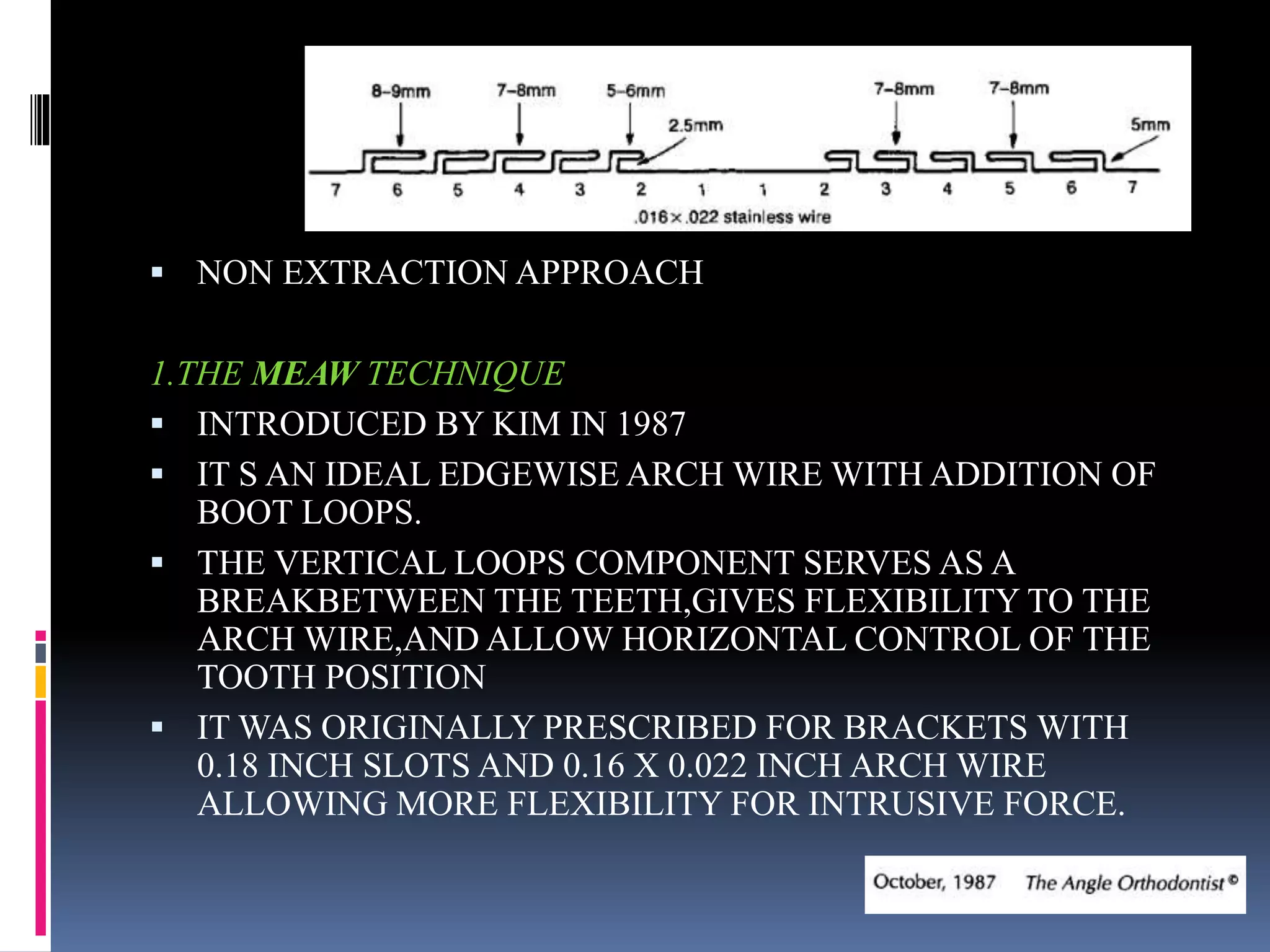

This document provides an overview of class III malocclusions, including definition, etiology, classification, clinical examination, and treatment approaches. It discusses pseudo and skeletal class III malocclusions. Treatment options covered include functional appliances like Frankel III regulator, chin cup, and face mask therapy. It also discusses camouflage treatment approaches like non-extraction and extraction methods. The goal of early interceptive treatment is preventing worsening and providing favorable growth. Functional appliances aim to redirect mandibular growth. Camouflage treatments disguise the underlying skeletal deformity through dental movements.


































































