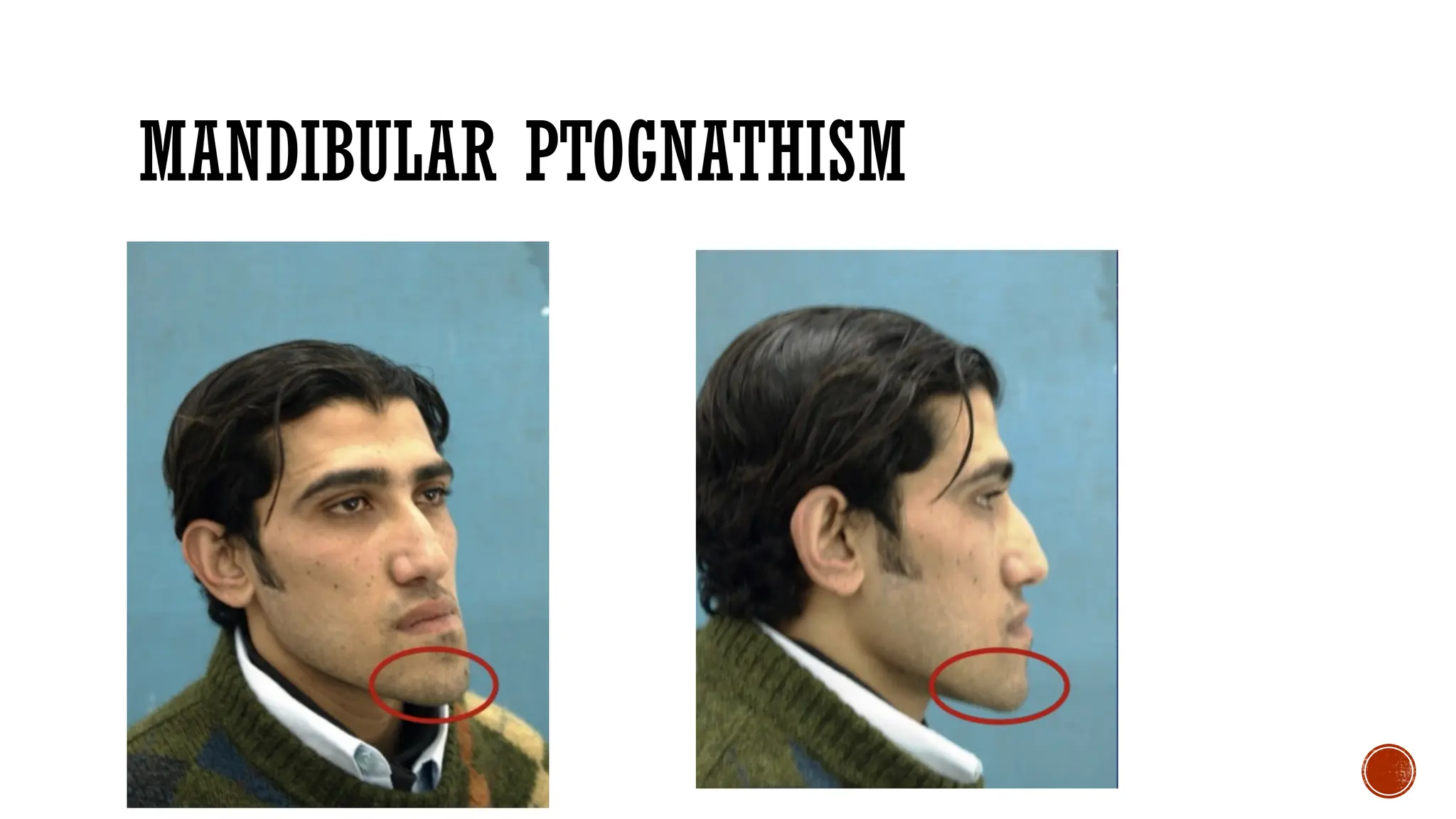
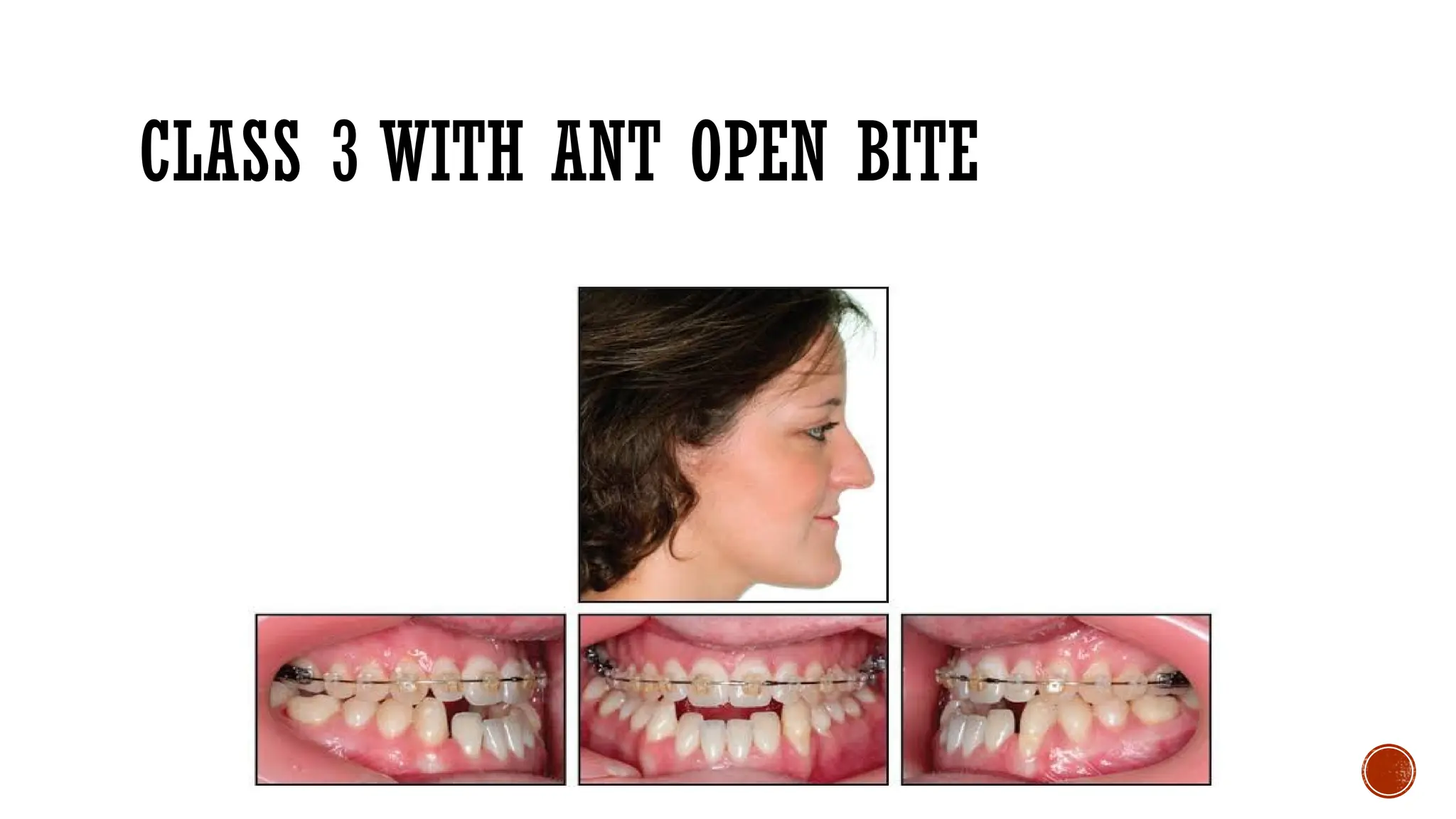
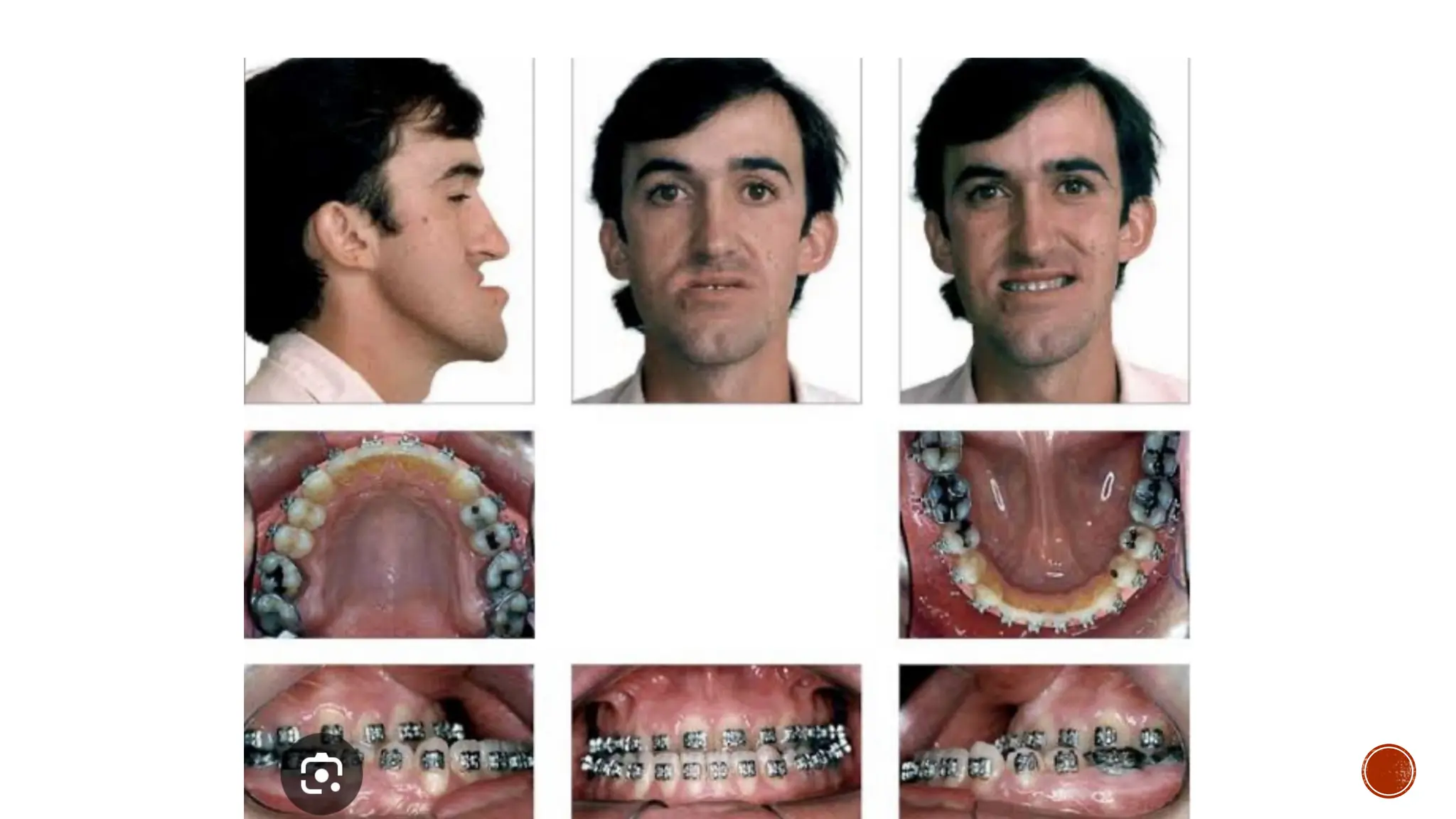
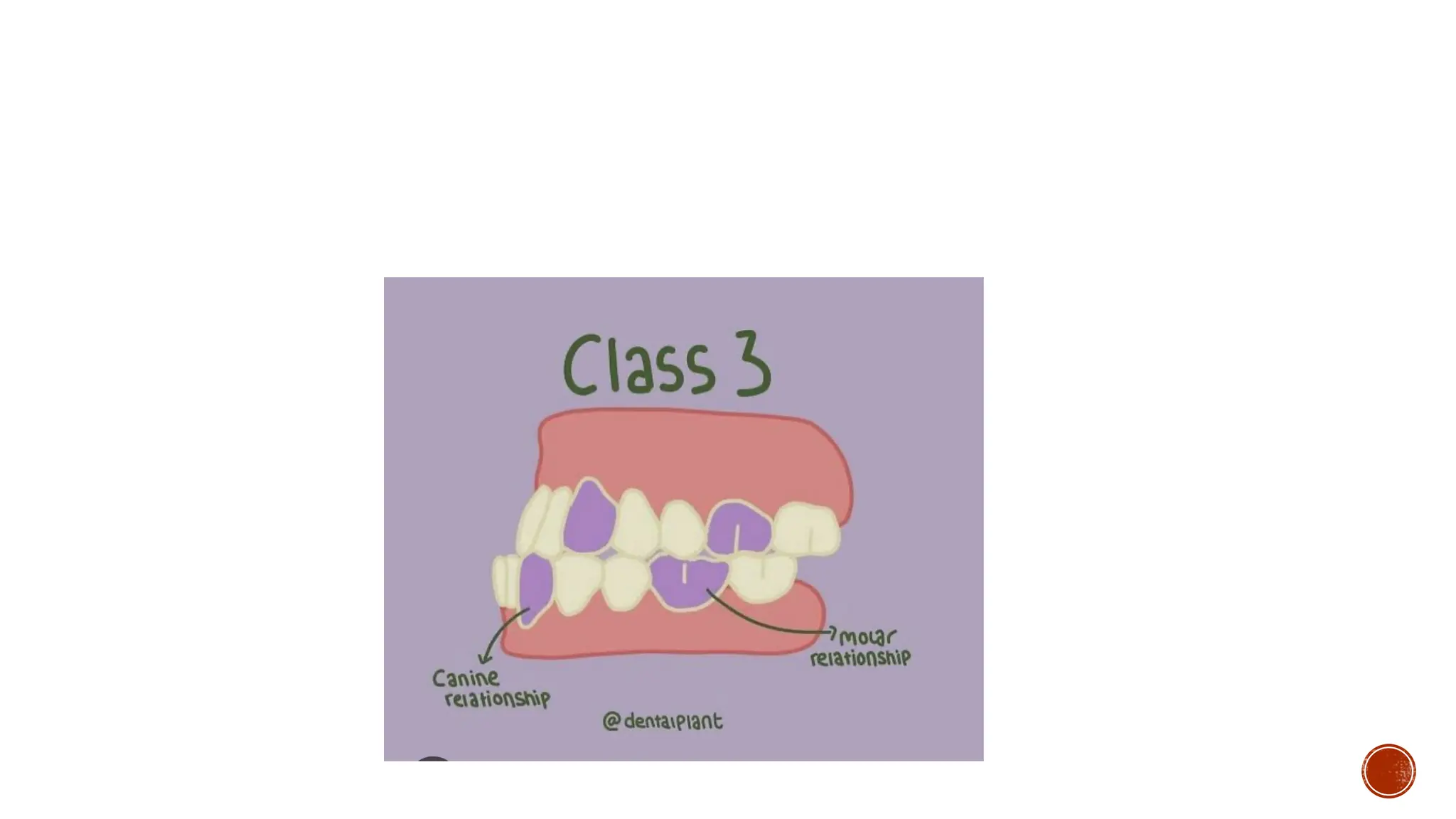
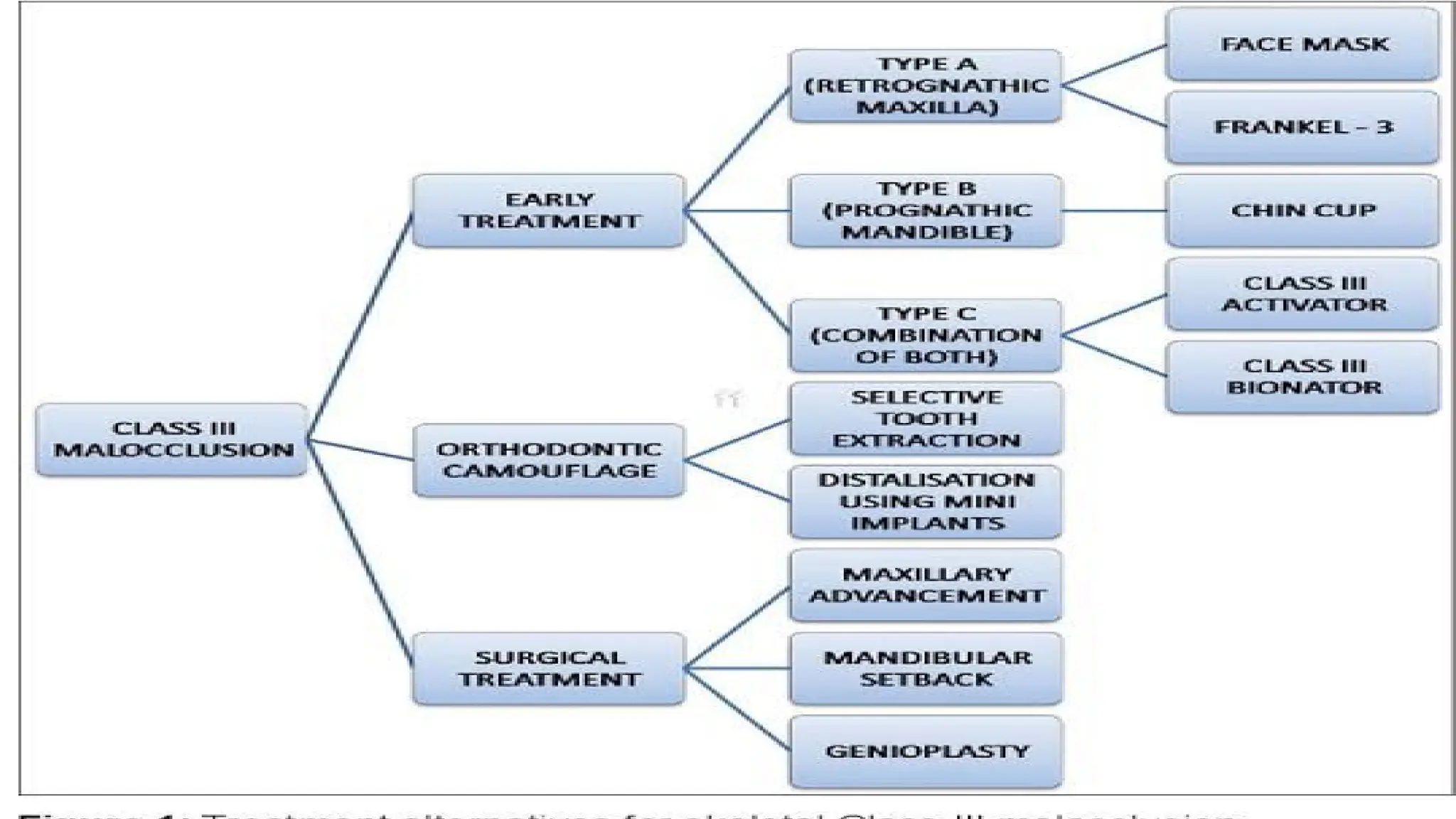
Class III malocclusion, characterized by the lower jaw protruding ahead of the upper jaw, is prevalent among various ethnic groups, with rates ranging from 1% to 8%. Its etiology includes genetic and environmental factors, as well as conditions like cleft lip and palate, presenting with specific clinical features. Diagnosis involves history, clinical examination, and records, with treatment options like face masks and chin cups to redirect jaw growth.


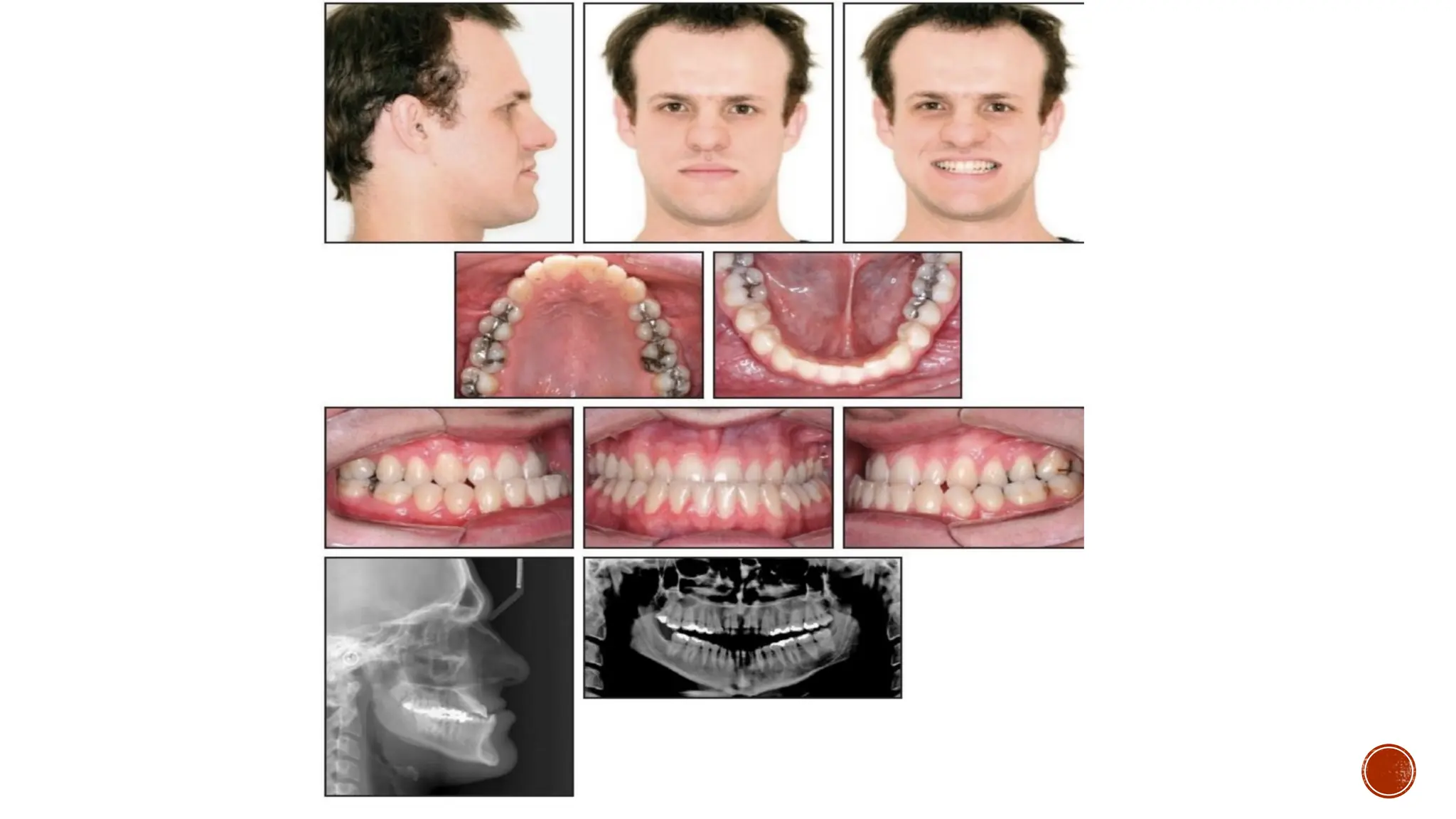
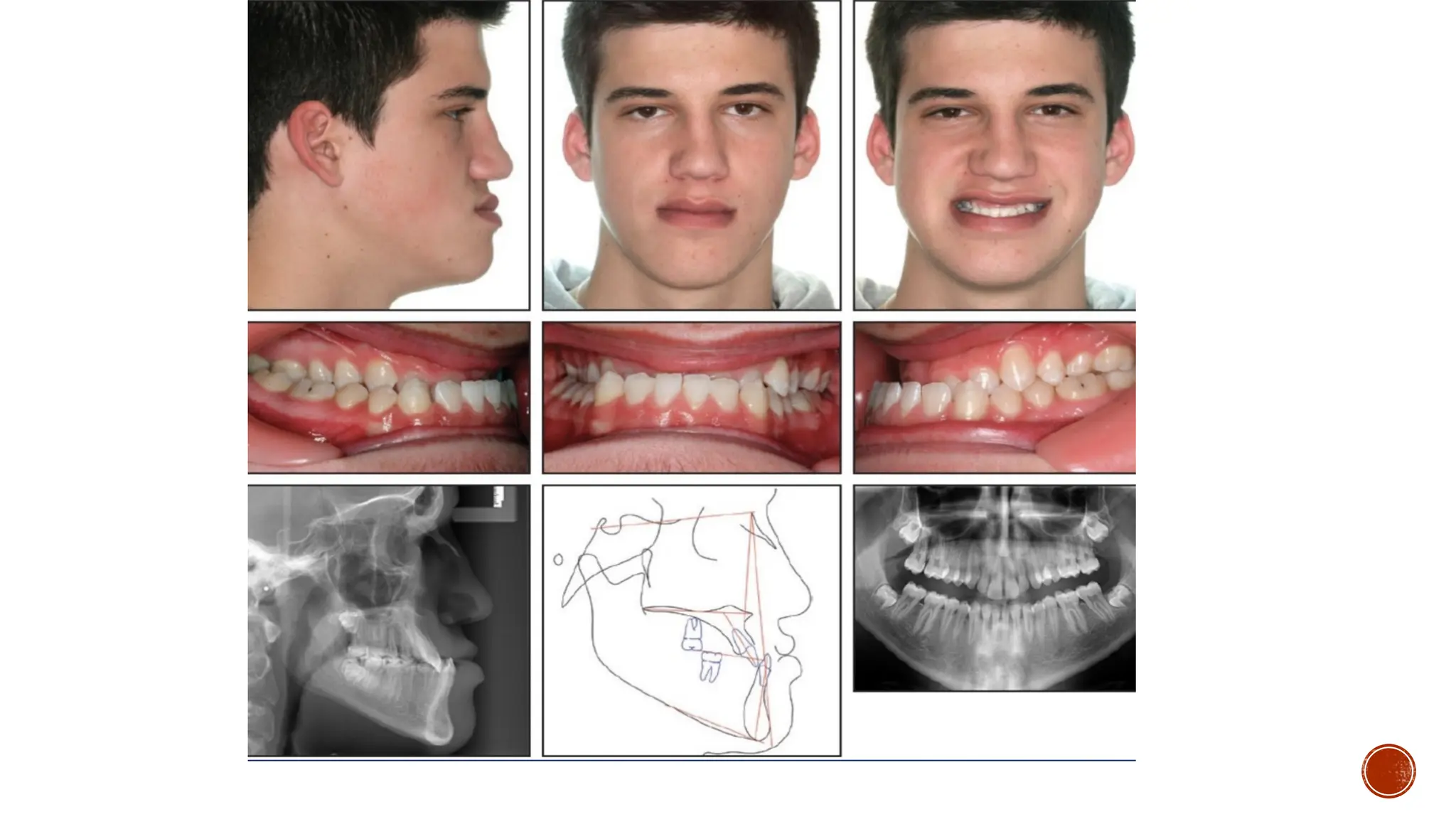
![ORTHODONTIC CAMOUFLAGE
Depending on the malocclusion extraction can be doneas follows:• Two lower
premolars or a mandibular incisor> All four premolars> Maxillary 2nd and
mandibular 1st premolars> Mandibular second molars[By Jiuxiang Lin, Angle
Orthodontist 2006;76(2)]](https://image.slidesharecdn.com/class3copycopycopycopy-241106214308-d643ddc0/75/Class-3-malocclusion-class-III-malocclusion-profit-13-2048.jpg)