Download to read offline


![The American Journal of GASTROENTEROLOGY VOLUME 105 | JANUARY 2010 www.amjgastro.com
76
REVIEW
Petrov and Windsor
6. Mole DJ, Olabi B, Robinson V et al. Incidence of individual organ
dysfunction in fatal acute pancreatitis: analysis of 1024 death records.
HPB 2009;11:166–70.
7. Lankisch PG. Natural course of acute pancreatitis: what we know today and
what we ought to know for tomorrow. Pancreas 2009;38:494–8.
8. Buter A, Imrie CW, Carter CR et al. Dynamic nature of early organ dysfunction
determines outcome in acute pancreatitis. Br J Surg 2002;89:298–302.
9. Johnson CD, Abu-Hilal M. Persistent organ failure during the first week as
a marker of fatal outcome in acute pancreatitis. Gut 2004;53:1340–4.
10. Acute Pancreatitis Classification Working Group. Revision of the Atlanta
classification of acute pancreatitis (3rd revision). www. pancreasclub.com/
resources/AtlantaClassification.pdf Accessed 1 April 2009.
11. Pannala R, Kidd M, Modlin IM. Acute pancreatitis: a historical perspective.
Pancreas 2009;38:355–66.
12. Gloor B, Müller CA, Worni M et al. Late mortality in patients with severe
acute pancreatitis. Br J Surg 2001;88:975–9.
13. Garg PK, Madan K, Pande GK et al. Association of extent and infection
of pancreatic necrosis with organ failure and death in acute necrotizing
pancreatitis. Clin Gastroenterol Hepatol 2005;3:159–66.
14. Beger HG, Rau BM. Severe acute pancreatitis: clinical course and manage-
ment. World J Gastroenterol 2007;13:5043–51.
15. Xue P, Deng LH, Zhang ZD et al. Infectious complications in patients with
severe acute pancreatitis. Dig Dis Sci 2008; [e-pub ahead of print].
16. Vege SS, Gardner TB, Chari ST et al. Low mortality and high morbidity
in severe acute pancreatitis without organ failure: a case for revising the
Atlanta classification to include “moderately severe acute pancreatitis”.
Am J Gastroenterol 2009;104:710–5.
17. Talukdar R, Vege SS, Chari ST et al. Moderately severe acute pancreatitis:
a prospective validation study of this new subgroup of acute pancreatitis.
Pancreatology 2009;9:434.
18. De-Madaria E, Soler G, Martinez J et al. Update of the Atlanta classification
of severity of acute pancreatitis: should a moderate category be included?
Pancreatology 2009;9:433–4.
19. Büchler MW, Gloor B, Müller CA et al. Acute necrotizing pancreatitis: treat-
ment strategy according to the status of infection. Ann Surg 2000;232:619–26.
20. Lytras D, Manes K, Triantopoulou C et al. Persistent early organ failure:
defining the high-risk group of patients with severe acute pancreatitis?
Pancreas 2008;36:249–54.
21. Le Mée J, Paye F, Sauvanet A et al. Incidence and reversibility of organ fail-
ure in the course of sterile or infected necrotizing pancreatitis. Arch Surg
2001;136:1386–90.
22. Isenmann R, Rau B, Beger HG. Early severe acute pancreatitis: characteris-
tics of a new subgroup. Pancreas 2001;22:274–8.
23. Tao HQ, Zhang JX, Zou SC. Clinical characteristics and management of
patients with early acute severe pancreatitis: experience from a medical
center in China. World J Gastroenterol 2004;10:919–21.
24. Petrov MS, van Santvoort HC, Besselink MG et al. Enteral nutrition
and the risk of mortality and infectious complications in patients with
severe acute pancreatitis: a meta-analysis of randomized trials. Arch Surg
2008;143:1111–7.
25. Windsor JA. Minimally invasive pancreatic necrosectomy. Br J Surg
2007;94:132–3.
26. Petrov MS. Meta-analyses on the prophylactic use of antibiotics in acute
pancreatitis: many are called but few are chosen. Am J Gastroenterol
2008;103:1837–8.
27. Cavallini G, Frulloni L. Somatostatin and octreotide in acute pancreatitis:
the never-ending story. Dig Liver Dis 2001;33:192–201.
28. Abu-Zidan FM, Windsor JA. Lexipafant and acute pancreatitis: a critical
appraisal of the clinical trials. Eur J Surg 2002;168:215–9.
29. Ishikawa K, Idoguchi K, Tanaka H et al. Classification of acute pancreatitis
based on retroperitoneal extension: application of the concept of
interfascial planes. Eur J Radiol 2006;60:445–52.
30. Bradley EL III. Confusion in the imaging ranks: time for a change?
Pancreas 2006;33:321–2.
31. Frey CF. Classification of pancreatitis: state-of-the-art, 1986. Pancreas
1986;1:62–8.
tives of the revision of the Atlanta classification, which are to
improve clinical assessment, facilitate communication between
treating physicians and promote standardization for reporting
clinical studies.
ACKNOWLEDGMENTS
We are indebted to Professor Peter A. Banks (Brigham and
Women’s Hospital, Harvard Medical School, Boston, MA) for
helpful discussion. Dr. Maxim S. Petrov is supported by the
Kenneth Warren Foundation of the International
Hepato-Pancreato-Biliary Association.
CONFLICT OF INTEREST
Guarantor of the article: Maxim S. Petrov, MD, MPH.
Specific author contributions: Planning, conducting, and
drafting the manuscript: Maxim S. Petrov; drafting and critical
reviewing of the manuscript: John A. Windsor.
Financial support: None.
Potential competing interests: None.
REFERENCES
1. Bradley EL III. A clinically based classification system for acute pancrea-
titis. Summary of the International Symposium on Acute Pancreatitis,
Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993;128:586–90.
2. Vege SS, Chari ST. Organ failure as an indicator of severity of acute pancreatitis:
time to revisit the Atlanta classification. Gastroenterology 2005;128:1133–5.
3. Banks PA, Freeman ML. Practice guidelines in acute pancreatitis. Am J
Gastroenterol 2006;101:2379–400.
4. Pandol SJ, Saluja AK, Imrie CW et al. Acute pancreatitis: bench to the
bedside. Gastroenterology 2007;132:1127–51.
5. Flint R, Windsor JA. Early physiological response to intensive care as a
clinically relevant approach to predicting the outcome in severe acute
pancreatitis. Arch Surg 2004;139:438–43.
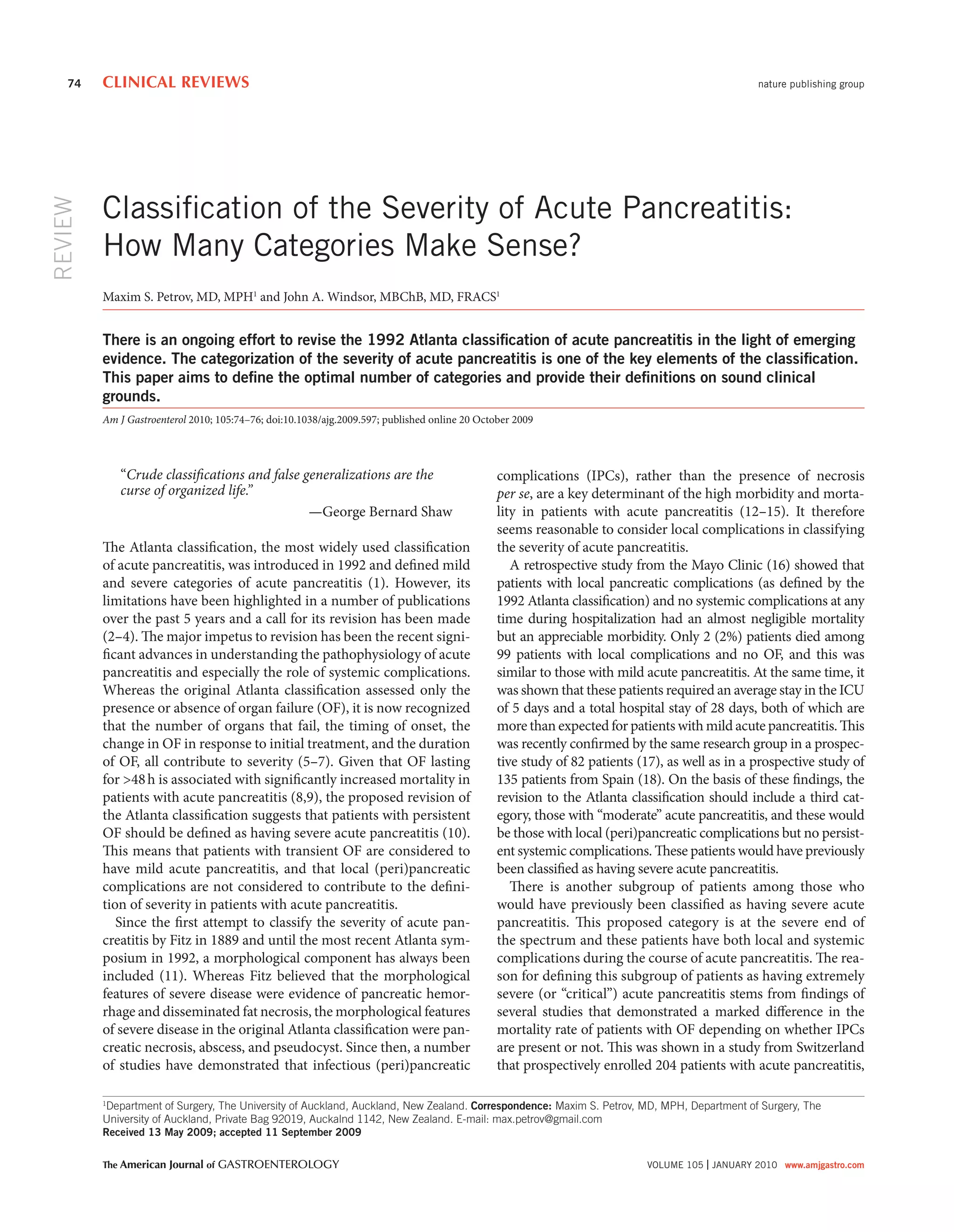
Table 1. Classification and definitions of four categories for
the severity of acute pancreatitis
Severity
category
Local complications Systemic
complications
Mild No (peri)pancreatic
complication
and No organ failure
Moderatea
Sterile (peri)pancreatic
complication
or Transient organ
failure
Severea
Infectious (peri)pancreatic
complication
or Persistent organ
failure
Critical Infectious (peri)pancreatic
complication
and Persistent organ
failure
a
Severity is graded on the basis of more severe local or systemic complication
(e.g., sterile pancreatic necrosis without organ failure has to be graded as
“moderate”; sterile pancreatic necrosis with persistent organ failure has to be
graded as “severe”).](https://image.slidesharecdn.com/clasificaciondemaximpetrov-150617003022-lva1-app6891/85/Clasificacion-de-Maxim-Petrov-3-320.jpg)

- The 1992 Atlanta classification of acute pancreatitis defined mild and severe categories based on organ failure, but recent evidence shows this is too simplistic. - A proposed revision suggests classifying patients based on transient versus persistent organ failure, with persistent organ failure defining severe acute pancreatitis. - There is also a need to distinguish patients with local complications from those with both local and systemic complications, as mortality is much higher in the latter group. This suggests acute pancreatitis should be classified into mild, moderate, and severe/critical categories.























































































