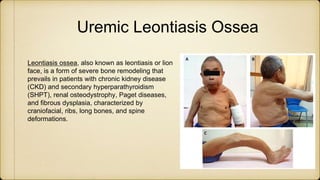
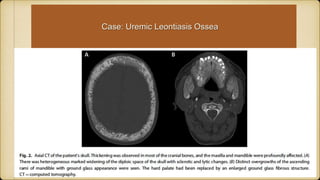
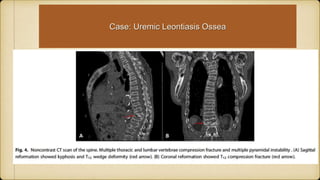
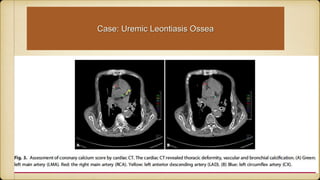
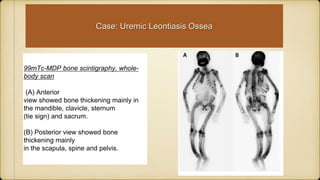
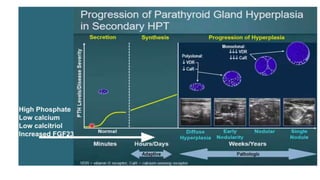
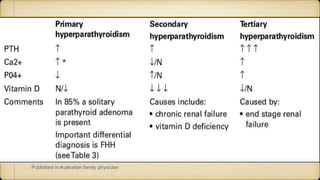
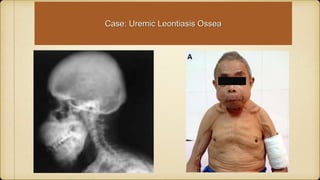
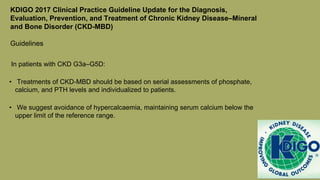
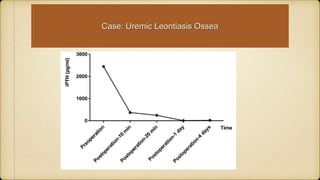
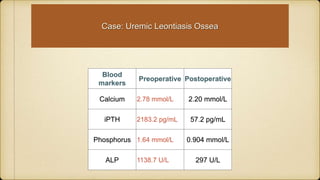
This document discusses a case of uremic leontiasis ossea in a 62-year-old male with chronic kidney disease and secondary hyperparathyroidism. He presented with severe bone deformities and high parathyroid hormone levels. Tests found hyperplasia of the parathyroid glands. He underwent parathyroidectomy with removal of five glands, one being supernumerary. Post-operatively, his calcium, phosphorus, and parathyroid hormone levels improved significantly. The case demonstrates how prolonged secondary hyperparathyroidism can lead to severe bone deformities but can be treated with surgery.

































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















