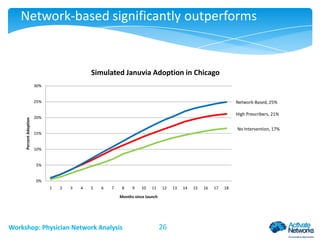
Download to read offline
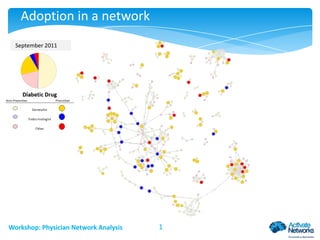
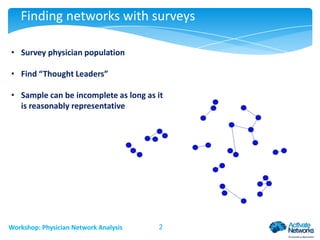
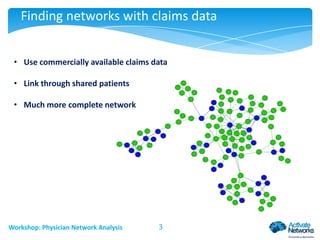
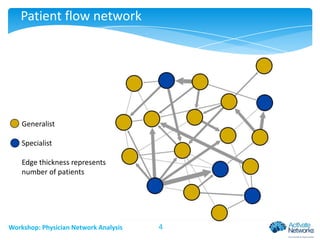
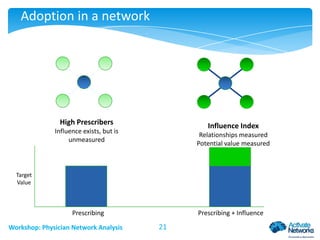
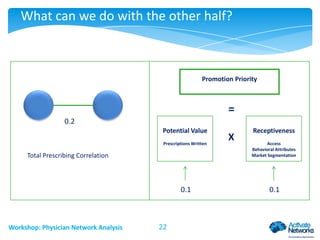
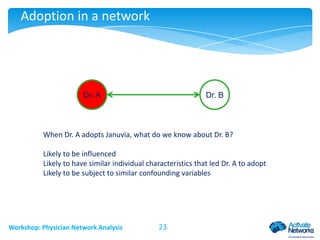
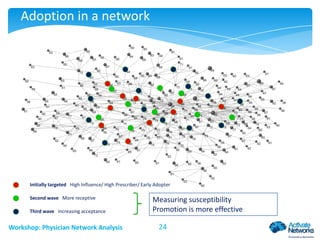
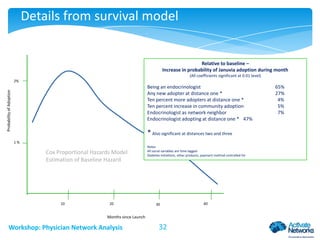
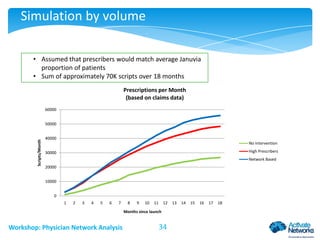
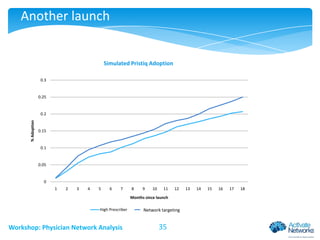


This document discusses analyzing physician networks and the adoption of new drugs. It provides examples of using claims data and surveys to map physician networks. Key topics covered include identifying influential physicians, examining how information and behaviors spread through networks, finding communities of practice, and using network analysis to predict how new drugs will diffuse. Network-based targeting of marketing is found to significantly outperform targeting based solely on prescribing volume. Network effects are shown to increase the probability that a physician will adopt a new drug.























































































