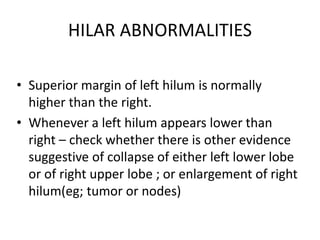
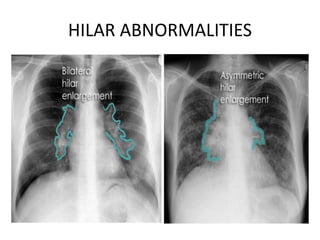
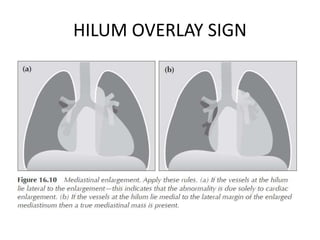
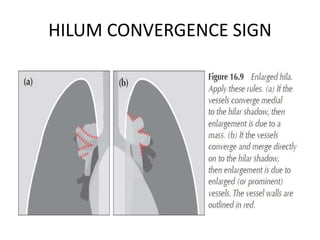
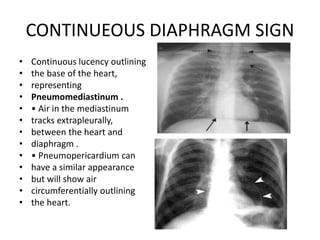
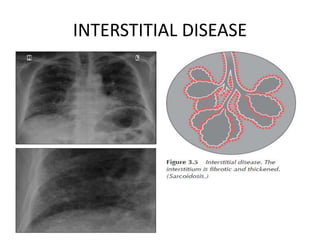
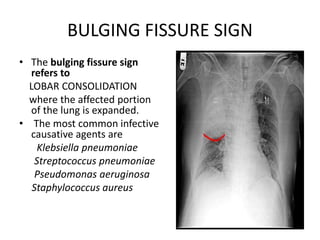
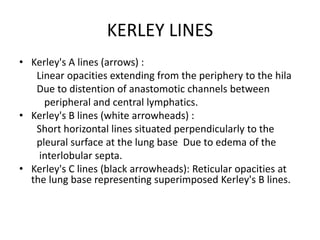
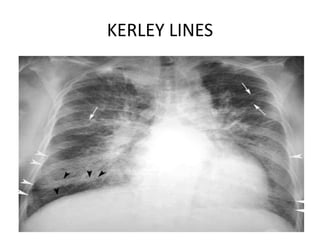
This chest x-ray report discusses various abnormalities that can be seen on a chest x-ray including hilar abnormalities, the hilum overlay sign, hilum convergence sign, and continuous diaphragm sign. Specific lung abnormalities are also described such as alveolar disease, interstitial disease, bulging fissure sign, lobar consolidation, Kerley lines, and a miliary pattern. Causes of a miliary pattern include tuberculosis, sarcoidosis, silicosis, histoplasmosis, and haemochromatosis.






![D/D OF MILIARY PATTERN
• TB (HAEMATOGENOUS)(lower lobe predominant due
to more perfusion)
[Primary TB present as U/L hilar lymphadenopathy]
• SARCOIDOSIS
• SILICOSIS (upper lobe predominant)
• HISTOPLASMOSIS
• HAEMOSIDEROSIS
• ALVEOLAR MICROLITHIASIS
• FAT EMBOLISM
• METASTASIS (sometimes)](https://image.slidesharecdn.com/chestx-ray-221227010043-b5e51658/85/CHEST-X-RAY-PPT-pptx-20-320.jpg)










































































