The document provides information on how to interpret a chest x-ray, including:
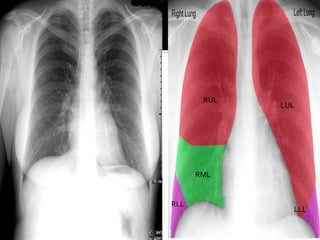
- The chest x-ray allows visualization of the heart, lungs, airways, blood vessels and chest bones.
- Different tissues show up differently on x-rays due to their absorption of the x-rays.
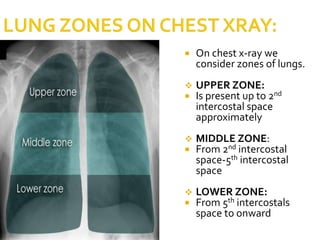
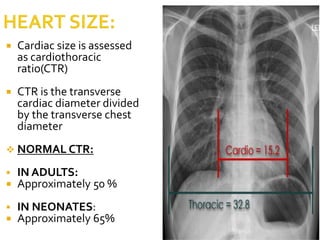
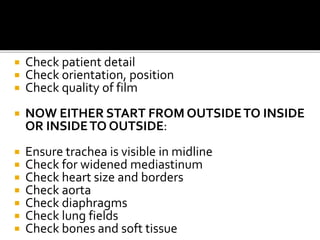
- When interpreting a chest x-ray, one should check for positioning, evaluate the lungs and heart size, examine bones and soft tissues, and look for any abnormalities.
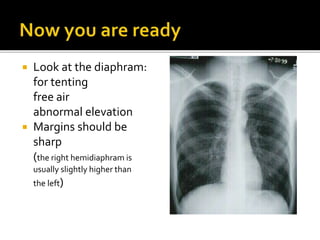
- Key aspects include assessing lung opacities, fractures, the diaphragm, and using the x-ray to help diagnose various chest pathologies.