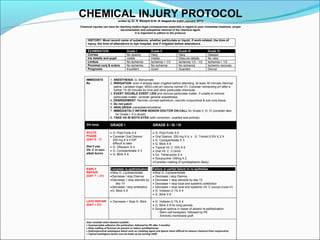
This document outlines a chemical injury protocol written by Dr. R. Banayot & Dr. N. Sargent for SJEH in January 2011. It discusses the importance of proper immediate treatment, documentation, and chemical removal to avoid far-reaching medico-legal consequences of chemical injuries. The protocol details examination and grading of injuries, immediate irrigation and treatment, acute and late phase management including medications and surgical options, and considerations for different grades of injury from I to IV.