CHEMICAL INJURIES
Oneof the true ophthalmic emergencies
Often result in significant ocular
morbidity and generally strike young
adults in the prime of life.
2nd
most common cause of work based
eye injuries at 12%.
4.
EPIDEMIOLOGY
2/3rd
in youngmales.
2/3rd
at Workplace vs home
Alkali > Acid
2/3rd
are minor (gr. I & II) injuries
In India common d/t fire cracker
injuries,lime or after accidental injury with
holi colours
5.
Acid injury
Acidsdissociate into hydrogen ions and
anions in the cornea, e.g.: HCl= H+
+Cl-
The hydrogen molecule damages the
ocular surface by altering the pH, while
the anion causes protein denaturation,
precipitation, and coagulation .
Protein coagulation generally prevents
deeper penetration of acids.
MECHANISM
6.
Alkali injury
pHchanges: increase in pH , which
saponifies the fatty acid of cell
membranes leading to cell destruction.
Ulceration & proteolysis: Alkalies cause
stromal ulceration at two to three weeks
after injury this ulceration is though to be
due to various proteolytic enzymes.
Collagen synthesis defects
MECHANISM
7.
• Roper-Hall/ modifiedHughes classification
• Degree of corneal involvement
• Limbal ischemia.
• Dua classification
• Limbal involvement (in clock hours)
• Percentage of conjunctival involvement.
In a randomized controlled trial of acute burns, the Dua classification
was found to be superior to the Roper-Hall in predicting outcome in
severe burns. However, both classification schemes are commonly
employed in daily practice.
CLASSIFICATION OF CHEMICAL INJURIES
8.
DUAS CLASSIFICATION
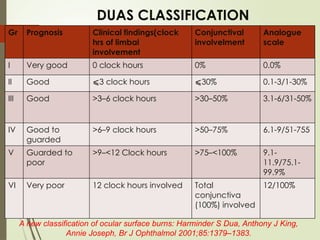
Gr PrognosisClinical findings(clock
hrs of limbal
involvement
Conjunctival
involvelment
Analogue
scale
I Very good 0 clock hours 0% 0.0%
II Good ⩽3 clock hours ⩽30% 0.1-3/1-30%
III Good >3–6 clock hours >30–50% 3.1-6/31-50%
IV Good to
guarded
>6–9 clock hours >50–75% 6.1-9/51-755
V Guarded to
poor
>9–<12 Clock hours >75–<100% 9.1-
11.9/75.1-
99.9%
VI Very poor 12 clock hours involved Total
conjunctiva
(100%) involved
12/100%
A new classification of ocular surface burns: Harminder S Dua, Anthony J King,
Annie Joseph, Br J Ophthalmol 2001;85:1379–1383.
9.
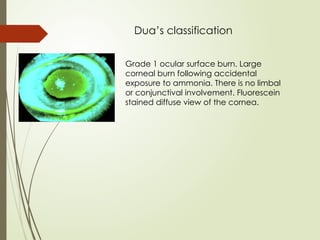
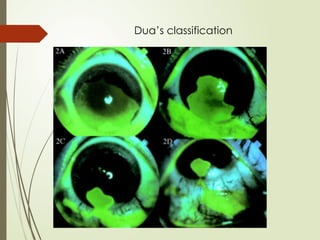
Dua’s classification
Grade 1ocular surface burn. Large
corneal burn following accidental
exposure to ammonia. There is no limbal
or conjunctival involvement. Fluorescein
stained diffuse view of the cornea.
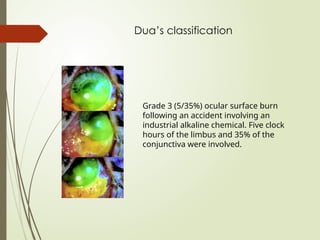
Dua’s classification
Grade 3(5/35%) ocular surface burn
following an accident involving an
industrial alkaline chemical. Five clock
hours of the limbus and 35% of the
conjunctiva were involved.
12.
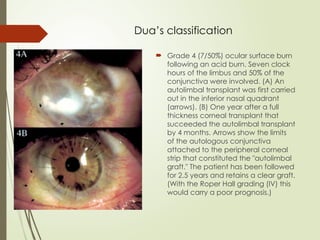
Dua’s classification
Grade4 (7/50%) ocular surface burn
following an acid burn. Seven clock
hours of the limbus and 50% of the
conjunctiva were involved. (A) An
autolimbal transplant was first carried
out in the inferior nasal quadrant
(arrows). (B) One year after a full
thickness corneal transplant that
succeeded the autolimbal transplant
by 4 months. Arrows show the limits
of the autologous conjunctiva
attached to the peripheral corneal
strip that constituted the "autolimbal
graft." The patient has been followed
for 2.5 years and retains a clear graft.
(With the Roper Hall grading (IV) this
would carry a poor prognosis.)
13.
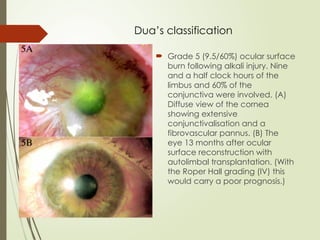
Dua’s classification
Grade5 (9.5/60%) ocular surface
burn following alkali injury. Nine
and a half clock hours of the
limbus and 60% of the
conjunctiva were involved. (A)
Diffuse view of the cornea
showing extensive
conjunctivalisation and a
fibrovascular pannus. (B) The
eye 13 months after ocular
surface reconstruction with
autolimbal transplantation. (With
the Roper Hall grading (IV) this
would carry a poor prognosis.)
14.
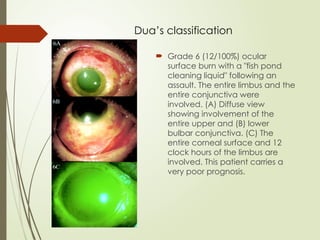
Dua’s classification
Grade6 (12/100%) ocular
surface burn with a "fish pond
cleaning liquid" following an
assault. The entire limbus and the
entire conjunctiva were
involved. (A) Diffuse view
showing involvement of the
entire upper and (B) lower
bulbar conjunctiva. (C) The
entire corneal surface and 12
clock hours of the limbus are
involved. This patient carries a
very poor prognosis.
15.
MANAGEMENT
Management ofthe case of chemical
burns can be divided into:
Immediate / Emergency Treatment
Early acute phase treatment
Intermediate term treatment
Late rehabilitation treatment
16.
MANAGEMENT
Immediate /Emergency treatment:
1. Irrigation with NS/water/BSS for atleast 30 mins. or
till pH turns neutral.
2. Eyelid immobilization with eyelid speculum or
retractor.
3. Instillation of topical anaesthesia.
4. Removal of particulate matter/debris after double
eversion of lids.
17.
MANAGEMENT
Early AcutePhase treatment:
Broadly classified into :
Those promoting reepithelization / transdifferntiation:
Tear substitutes, Bandage soft contact lens, Fibronectin, Epidermal growth
factor, Retinoic Acid.
Those supporting repair and minimizing ulceration:
Ascorbate, Collagenous inhibtors like sodium EDTA 0.2 M, calcium EDTA 0.2 M,
penicillum 0.2 M and 10 % to 20%acetylcystine.
Those controlling inflammation.
18.
Early AcutePhase treatment:
Aim of treatment is to restore the cornea with normal epithelium and a clear
stroma by decreasing the inflammation and enhancing the healing.
Treatment after irrigation is as follows:
1. Topical steroids 2 hourly
(inhibits PMN proliferation and function)
2. Topical sodium citrate 10% 2 hourly
(inhibits PMN degranulation by Ca chelation)
3. Tetracycline 1% ointment QID
(inhibits collagenase enzyme by chelating with Zn)
4. Oral sodium ascorbate 500mg QID
(promotes collagen synthesis)
5. Topical sodium ascorbate 20% 2 hourly
(promotes collagen synthesis)
6. Tear substitutes 2 hourly
(promotes epithelial healing)
7. Cycloplegics TDS or BD
(relieves pain)
8. Topical/oral antiglaucoma therapy, if needed
9. Conjunctival/tenons advancement for grade-IV.
(Improves vascularization)
19.
MANAGEMENT
Intermediate Phasetreatment:
Conjunctival / Tenons advancement : It is based on the
principle of suturing vital connective tissue in the orbit to
reestablish limbal vascularity and to facilitate
epithelization.
Tissue adhesives: They are used in small corneal perforations, whereas
an emergency patch graft or therapeutic PK is done for large
perforations.
Amniotic membrane transplantation
20.
MANAGEMENT
Late RehabilitationPhase:
Impending or actual perforation
1. Tissue adhesives for <1mm perforations
2. Tectonic keratoplasty
Vascularised Cornea
1. Limbal stem cell transplantation followed by
Penetrating keratoplasty (PK) or Lamellar keratoplasty (LK) after 6 months.
2. Large PK or large LK
3. Keratoprosthesis in Bilateral cases.
For symblepharon/cicatrisation of conjunctiva
Amniotic membrane transplant/mucus membrane transplant can be done.
21.
REFERENCES
Dua HS,King AJ, Joseph A. A new classification of ocular surface
burns. Br J Ophthalmol. 2001 Nov;85(11):1379-83. doi:
10.1136/bjo.85.11.1379. PMID: 11673310; PMCID: PMC1723789.
DOS Times: Chemical Injuries of the Eye
Dr. Tishu Saxena MS, Dr. Radhika Tandon MD, DNB, FRC Ophth., FRCS
Ed, Dr. Jeewan S. Titiyal MD
Kanski's Clinical Ophthalmology, Tenth Edition: Textbook by John
F. Salmon
https://doi.org/10.1038/s41433-020-1026-6: Chemical eye injury:
pathophysiology, assessment and management
Harminder S. Dua ● Darren Shu Jeng Ting ● Ahmed Al Saadi ● Dalia
G. Said
22.
MANAGEMENT
Late RehabilitationPhase:
Impending or actual perforation
1. Tissue adhesives for <1mm perforations
2. Tectonic keratoplasty
Vascularised Cornea
1. Limbal stem cell transplantation followed by
Penetrating keratoplasty (PK) or Lamellar keratoplasty (LK) after 6 months.
2. Large PK or large LK
3. Keratoprosthesis in Bilateral cases.
For symblepharon/cicatrisation of conjunctiva
Amniotic membrane transplant/mucus membrane transplant can be done.
Editor's Notes
#5 The severity of a chemical injury is related to properties of chemical, area of affected ocular surface, duration of exposure and related effects such as thermal damage.
The mechanism of injury differs slightly between acids and alkali.
#18 During first 10 days
of an injury, topical corticosteroids should be given every
6 hours. It helps to reduce inflammatory cells infiltrating
the corneal stroma which are a source of the proteolytic
enzymes responsible for corneal ulceration. If corneal
epithelium is not intact after 10 days of injury, then the
topical corticosteroids should be rapidly tapered off as it
is known to inhibit the reparative process taking place in
eye.
#19 The management goals during this stage are mainly, structural reconstruction and ocular surface restoration.
Along with the continued medical treatment, surgical modalities are the mainstay of treatment in this stage of ocular burns. The various stategies includes: