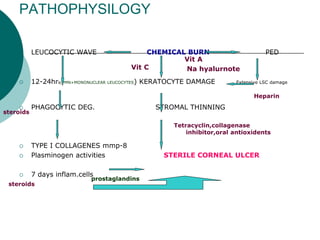
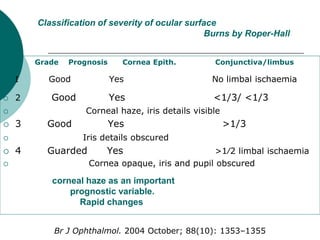
Chemical burns to the eye from industrial accidents or cleaning products can cause permanent vision loss by damaging the cornea and anterior eye structures. Alkali substances like lye and ammonia tend to penetrate more deeply and cause more extensive tissue necrosis, while acids often cause more superficial burns. The severity of injury is classified based on the extent of epithelial defects and limbal stem cell damage. Immediate irrigation is critical. Treatment focuses on reducing inflammation, promoting re-epithelialization, and addressing complications like pseudopterygium, symblepharon, or limbal stem cell deficiency that may require surgical intervention to restore ocular surface integrity and vision. Outcomes depend on the chemical agent, depth of injury, and success of