Download to read offline




![Ann Emerg Med. 2018 Nov 14. pii: S0196-0644(18)31326-X. doi:
10.1016/j.annemergmed.2018.09.033. [Epub ahead of print]
Older Blood Is Associated With Increased Mortality and Adverse Events in Massively
Transfused Trauma Patients: Secondary Analysis of the PROPPR Trial
• CONCLUSION:
• Increasing quantities of older packed RBCs are
associated with increased likelihood of 24-hour
mortality in trauma patients receiving massive packed
RBC transfusion (≥10 units), but not in those who
receive fewer than 10 units.
33](https://image.slidesharecdn.com/2-190516132724/85/Challenging-hemorrhagic-shock-resuscitation-guidelines-33-320.jpg)





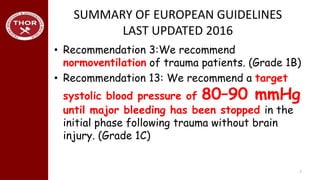
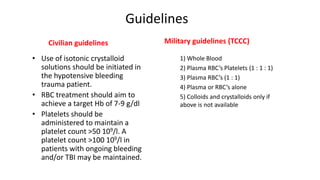
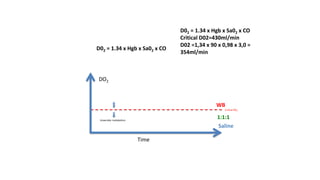
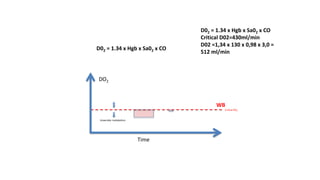
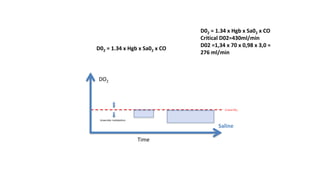
The document discusses guidelines for resuscitation of hemorrhagic shock. It summarizes some key recommendations from European guidelines from 2016, which recommend initiation of isotonic crystalloid fluids for hypotensive bleeding trauma patients and a target hemoglobin level of 7-9 g/dL. It also notes that military guidelines recommend use of whole blood, plasma, red blood cells, and platelets in a 1:1:1 ratio as the preferred resuscitation strategy over crystalloids alone. The document questions whether the European guideline recommendations are well-aligned with the pathophysiology of hemorrhagic shock.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















