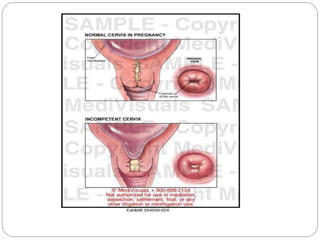

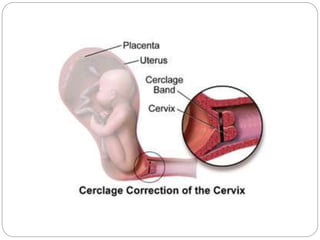

Cervical incompetence, also known as cervical insufficiency, is a pregnancy condition where the cervix dilates and effaces prematurely, potentially leading to miscarriage or preterm birth. It occurs in about 1% of pregnancies and can be diagnosed through history, internal examinations, and ultrasound. Management involves cervical cerclage for reinforcement, along with specific postoperative care and monitoring for potential complications.



































































